Marine transportation safety investigation report M17A0390
Grounding
Bulk carrier SBI Carioca
Belledune, New Brunswick
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content.
-
Table of contents
Summary
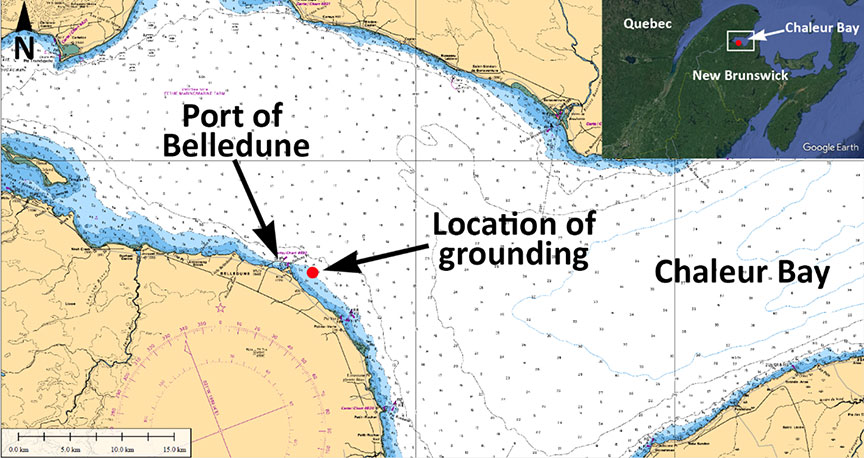
On 11 October 2017, at 0720 Atlantic Daylight Time, the bulk carrier SBI Carioca, with a pilot and 22 crew members on board, ran aground while approaching the pier at the Port of Belledune, New Brunswick, in Chaleur Bay. The vessel was refloated on the next high tide with the assistance of 2 tugs. No damage or pollution was reported. No injuries were reported.
1.0 Factual information
1.1 Particulars of the vessel
Table 1. Particulars of the vessel
| Name of vessel | SBI Carioca |
|---|---|
| Port of registry | Majuro |
| Flag | Marshall Islands |
| Type | Bulk carrier |
| Gross tonnage | 43 301 |
| Length | 229 m |
| Breadth | 32.26 m |
| Propulsion | 1 diesel engine (9932 kW) driving a fixed-pitch propeller |
| Cargo | 65 962.14 metric tonnes of petroleum coke |
| Crew | 22 |
| Registered owner | SBI Carioca Shipping Company Ltd., Majuro, Marshall Islands |
1.2 Description of the vessel
The SBI Carioca (Figure 1) is a dry bulk cargo vessel of steel construction with machinery space and accommodations located aft. The vessel has 7 cargo holds and is propelled by a diesel engine driving a fixed-pitch propeller. The vessel is not equipped with bow or stern thrusters.

The bridge is equipped with the required navigational equipment, including a 10 cm wavelength radar that is located right of the centre console, and a 3 cm wavelength radar that is located to the left of the console. The bridge is also fitted with 2 gyrocompasses, a magnetic compass, a depth sounder, and 2 very high frequency (VHF) radiotelephones incorporated into its Global Maritime Distress and Safety System (GMDSS).
The vessel is equipped with a differential global positioning system (DGPS), and 2 electronic chart display and information systems (ECDIS), one alongside each radar. A repeater monitor for the ECDIS is mounted on the deckhead above the centre console. A voyage data recorder (VDR) is also installed on board.
1.3 History of the voyage
On 05 October 2017, the SBI Carioca departed Newport News, Virginia, for Belledune, New Brunswick, with 65 962 metric tonnes of petroleum coke (petcoke) in the cargo holds and 22 crew members on board.
On 11 October, the vessel was making its approach westward to the Port of Belledune, New Brunswick (Appendix A), to arrive on the morning tide. The intention was to meet the pilot at the pilot boarding station; the pilot would then board the SBI Carioca and pilot the vessel to the northernmost pier at the port to discharge the cargo.
At 0530,Footnote 1 the master of the SBI Carioca contacted the master of the Atlantic TeakFootnote 2 by VHF radiotelephone to discuss pilot boarding arrangements. At 0635, the master of the pilot boat informed the master of the SBI Carioca that the pilot was departing the port and en route to the SBI Carioca. The master responded that the SBI Carioca was about 0.5 nautical miles (nm) from the pilot boarding station.Footnote 3 The winds were blowing west-northwest at 25 knots, visibility was good, and the tide was rising, set to reach high tide at 0813. The vessel's draft was 12.65 m.
Because the pilot boarding station was not marked on any charts, the master ordered that the SBI Carioca proceed to an area approximately 1.5 nm northeast of the pier.
When the Atlantic Teak approached the SBI Carioca, the crew on board the Atlantic Teak observed that the SBI Carioca's pilot ladder was dragging in the water and requested that the crew of the SBI Carioca raise it. This delayed the pilot's boarding of the vessel by about 4 minutes. By the time the pilot was on the bridge, at 0655, the SBI Carioca was 0.9 nm northeast of the pier (Figure 2).

When the pilot arrived on the bridge, there was a brief exchange of vessel information between the master and the pilot. The pilot then called for hard to starboard; the vessel was too close to the pier and there would not be enough time for it to safely make its approach. Because the tide would be turning, the pilot initiated a circular manoeuvre that included numerous and varied course and speed alterations to position the vessel further to the east, in order to give the vessel more time and distance to set up its approach to the pier. At this time, the bridge team consisted of the master, the pilot, and a helmsman. The officer of the watch had left the bridge in order to raise flags on the ship's mast atop the vessel's wheelhouse.
By approximately 0702, the vessel had completed the apex of its circular manoeuvre and was making good a course of 160°. The pilot's priority was to slow the vessel down before making the turn for the approach to the northern pier, so he ordered the Atlantic Teak and the Atlantic SpruceFootnote 4 to make their lines fast fore and aft and begin slowing the vessel down while gradually turning to starboard. At this time, the SBI Carioca's speed over ground was 6.7 knots.
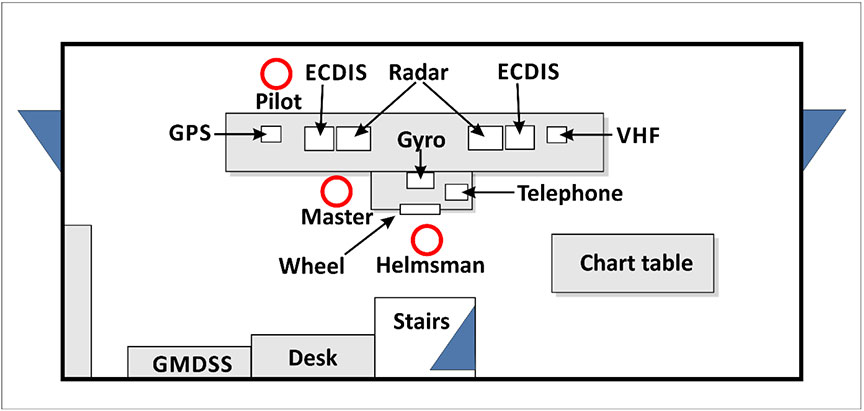
The pilot, who was standing ahead of the console and facing the wheelhouse windows (Figure 3), ordered numerous and varied manoeuvres for the vessel and tugs in an effort to slow the vessel down and alter its course toward the pier. The pilot was not monitoring the radars or ECDIS, and he issued helm orders without further communicating to other bridge team members his plans for an alternative approach to the pier.
At about 0720, the SBI Carioca ran aground in position 47 54.559′ N and 065 48.562′ W. Shortly thereafter, the pilot checked the radar for the first time, and at approximately 0729, the pilot realized the vessel was aground. The course made good when the vessel ran aground was 175°, and the speed over ground was about 3 knots.
The SBI Carioca was refloated at the next high tide with the assistance of the Atlantic Teak and the Atlantic Spruce. In accordance with requirements set by the company's selected classification society, a dive survey was conducted. No damage to the vessel or pollution was reported. No injuries were reported.
1.4 Personnel certification and experience
The master of the SBI Carioca held a valid unlimited master certificate, which was issued in 1999. He had sailed in various capacities on various vessels since 1996 and had worked with Claus-Peter Offen BulkschiffreedereiFootnote 5 as master since 2014. The master had sailed on the SBI Carioca since 22 September 2017 and had not been to the Port of Belledune before this occurrence.
At the time of the occurrence, the third officer held a valid second mate certificate (Officer in charge of the Navigational Watch (2nd Mate)) for the vessel and voyage he was engaged in. The third officer had sailed with the SBI Carioca for about 7 months and had 21 years of sailing experience.
The pilot held a valid Master Mariner certificate issued in Canada, and had been employed as a mariner in various capacities since 1966. He had worked as a pilot in the Dalhousie and Belledune area since 1989.
1.5 Vessel certification
The SBI Carioca was certified and equipped in accordance with existing regulations.
1.6 Pilot boarding station for and approaches to the Port of Belledune
The Port of Belledune is managed by the Belledune Port Authority (BPA), a federal entity whose role is to
facilitate and expand the movement of cargo through the Port of Belledune; provide good working, safe facilities; marine related services; and technologies that are competitive, safe, commercially variable and customer orientedFootnote 6
The BPA's office hours are from 0800 to 1600. The Port of Belledune has an after-hours cellphone number that crews can use to contact port personnel; however, the crew of the SBI Carioca did not have access to this number.
Although the Port of Belledune is not a compulsory pilotage port, the BPA requires all non-Canadian vessels to use the services of a licensed pilot.
Most pilot boarding stations, including some small ports in the immediate area, are clearly marked on navigational charts. Because the Port of Belledune's pilot boarding station was not marked on any chart, the ship's agent for the SBI Carioca forwarded to the master 2 possible locations where the pilot could board the vessel. These locations were derived from information forwarded by the BPA from its Port Information and Advice to Masters:
(A) Lat 47 56 N Long 65 48 W — 1.5 miles of Northeast breakwater (Pilot prefers this position)
(B) Lat 47 58 N Long 65 48 W — 3.0 miles Northeast of breakwaterFootnote 7
These coordinates are the same as those provided by the Admiralty Sailing Directions, towhich the crew of the SBI Carioca had access. However, these coordinates differ from the Canadian Sailing Directions, which state that “the pilot boat meets arriving vessels between 1.5 and 2 miles NE of the breakwater.”Footnote 8
Figure 4 shows the positions of the pilot boarding stations near the Port of Belledune. In the figure, “Pilot boarding station #1” refers to the boarding station designated as Position (A) in the Port of Belledune's Port Information and Advice to Masters. “Pilot boarding station #2” also refers to the boarding station designated as Position (A); this position is derived from coordinates, rather than from bearing and distance.

In preparation to meet the pilot and bring him on board the vessel, the second officer of the SBI Carioca entered the coordinates 47°55.61′ N and 065°48.43′ W into the passage plan on the ECDIS, placing the vessel on a bearing of 055° from the northern pier. Once the vessel reached this point (referred to in Figure 4 as “Pilot boarding station #3”), it was 1.5 nm from the northern pier.
The Port of Belledune is typically approached from northeast to southwest with a breakwater forming the northern pier. The eastern edge of the southern pier ends along a bank that is featured on charts as a 10 m depth contour extending 1.5 nm to the east. There are no navigation aids marking the bank. The pilot on board the SBI Carioca typically approached the northern pier from a distance of approximately 2 nm and relied solely on visual aids such as landmarks on the shore for navigation.
1.7 Atlantic Pilotage Authority
The Atlantic Pilotage Authority (APA) is a Crown corporation established in 1972, and is one of 4 authorities established under the Pilotage Act. The APA's mandate is to
establish, operate, maintain, and administer in the interests of safety an efficient pilotage service within designated regions. The Pilotage Act grants a monopoly to the Corporation to provide pilotage services in all Canadian waters in and around the provinces of Nova Scotia, New Brunswick, Prince Edward Island, Newfoundland and Labrador, and certain waters of Chaleur Bay in Quebec.Footnote 9
In 2011, the APA contracted a facilitator to conduct a Pilotage Risk Management Methodology (PRMM) study, or risk study, to assess whether the Port of Belledune should become a compulsory pilotage port or remain non-compulsory. The study had input from many stakeholders and interested parties, where risks and issues related to the port were identified. Following this study, the APA recommended that the Port of Belledune be designated a compulsory pilotage area. The APA's proposed amendments to the Atlantic Pilotage Authority Regulations were published in the Canada Gazette, Part I, in November 2013.Footnote 10
1.8 Passage planning
Under subsection 14(1) of the Charts and Nautical Publications Regulations, 1995, the master of a Canadian vessel
shall ensure, before proceeding to sea, that the intended voyage has been planned using the most recent editions of the charts, documents, and publications that are required to be used under sections 5 and 6 [of the Charts and Nautical Publications Regulations, 1995] and that account has been taken of the annex to IMO Resolution A.893(21), Guidelines for Voyage Planning.Footnote 11
The second officer of the SBI Carioca had filled out a passage plan for the voyage from Newport News, Virginia, to Belledune, New Brunswick, in accordance with the vessel's safety management system. The passage plan included all of the nautical publications, electronic charts, waypoints, and routes required for the voyage. For the approach to the Port of Belledune, the pilot boarding station was entered into the ECDIS at a point 1.5 nm northeast off the breakwater. The passage plan included 2 waypoints past the pilot boarding station: the breakwater and the northern pier.
The pilot did not have a formal passage plan, nor was one required. There was no agreement between the pilot and the master regarding the approach to the northern pier. The pilot initiated the vessel's circular manoeuvre almost immediately after arriving on the bridge, and a safe distance from the 10 m depth contour to the south was not discussed.
1.8.1 Settings on the electronic chart display and information system
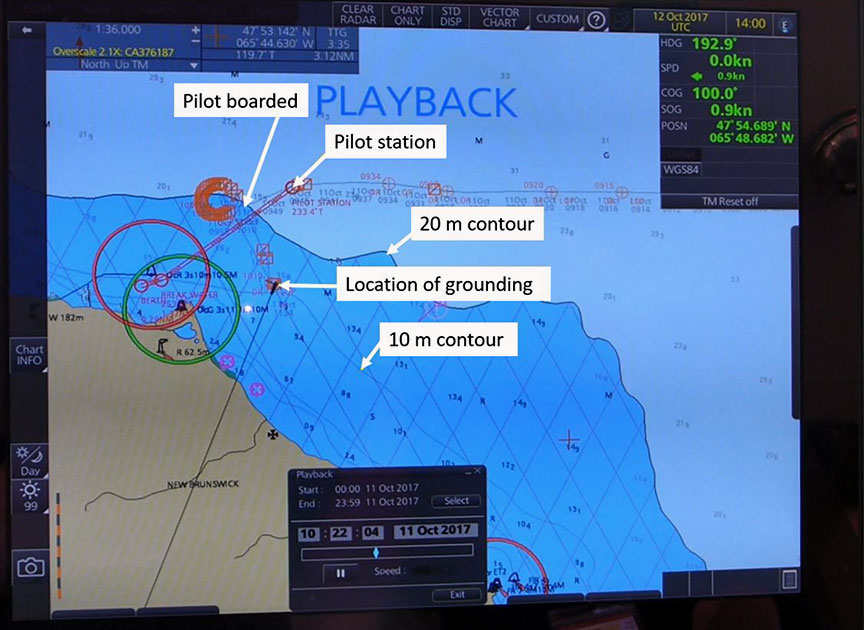
Charts normally use shading to identify depth contours of varying depths; the darker shades indicate shallower water.
The ECDIS on board the SBI Carioca has a variety of safety settings that the crew can select. These include settings to differentiate depth contours with shades of blue to indicate the depth contour above which the vessel can navigate safely. In this occurrence, the crew set all waters shallower than 20 m as dark blue, with no differentiation between the 20 m depth contour and the 10 m depth contour. The 10 m depth contour is less than the vessel's 12.65 m draft (Figure 5), even at high tide.Footnote 12
The SBI Carioca's passage plan indicated that 14 m had been selected as the safety depth contour, in accordance with the vessel's safety management system. The ECDIS did not have an alarm set to go off if the vessel crossed that safety depth contour.
1.9 Bridge resource management
Vessels must be navigated safely at all times, in compliance with the International Regulations for Preventing Collisions at Sea (COLREGs), and in a manner that will not harm the environment. Bridge resource management (BRM) is the management and use of all resources, human and technical, to ensure the safe completion of the voyage. Effective BRM mitigates the risk that an error on the part of 1 person, or a single-point of failure, will result in a dangerous situation.
Situational awareness and communication are key to effective BRM. Bridge team members have a responsibility to maintain overall situational awareness as well as to carry out their individual duties, especially during critical operations such as approaching a port. They also have a duty to work as a team to help prevent a single point of failure, which may occur when only 1 person is responsible for a safety-critical task. The exchange of information is necessary for the team to work together; ineffective communication can result in team members having different understandings of a situation as it unfolds.
At the time of the occurrence, the bridge team consisted of the helmsman, the master, and the pilot; the officer of the watch was not on the bridge. The helmsman was at the wheel, and the master was on the left side of the console and was monitoring the radar and ECDIS. The pilot had positioned himself ahead of the console, facing the wheelhouse windows, and was unable to see the vessel's ECDIS or the radar. From his position, the pilot ordered various manoeuvres. The pilot did not request information regarding the vessel's progress, and this information was not offered by other members of the bridge team or the crews of the tugs.
1.9.1 Situational awareness and mental models
Effective, safe decision making depends on the accuracy of one's situational awareness, which consists of perceiving elements in the environment in time and space, understanding what they mean, and predicting how they will change in the future.Footnote 13 Accurate situational awareness depends on the availability, clarity, and comprehensibility of external cues and information sources (e.g., physical, cognitive, or perceptual).
A person's overall understanding of a situation is based on experience, knowledge, and perception of external cues, which are used to develop what is known as a mental model of the situation. Mental models of an unfolding situation are difficult to change once they have been developed, particularly in a short period of time. New information must be provided (and identified) that is sufficiently noticeable and compelling to result in the person changing their mental model.
A shared mental model develops when all team members work as a cohesive team and have a common understanding of the task at hand. Under high workload conditions, a shared mental model among bridge team members that is based on data from secondary sources, such as a vessel's radar display and communication between bridge team members, become more important for safe navigation.
Mariners rely on a number of information sources (e.g., technological, physical, auditory, or visual) to inform their situational awareness and construct a mental model. This is especially the case in situations involving high workload, for example when under time constraints due to the turning of the tide and less-than-favourable weather conditions.
Although the vessel was equipped with electronic navigation aids that were monitored by a member of the bridge team, the pilot on board the SBI Carioca developed his mental model of the approach based on his extensive experience piloting vessels to the port, and used visual cues to verify the situation. The master's mental model relied on his previous experience approaching other ports under the conduct of a pilot, so the master expected that the pilot, with greater local knowledge and experience in navigating vessels into his home port, could negotiate the approach without his input.
In this occurrence, the pilot's priority was to reset the approach to gain a greater distance from the breakwater and the northern pier, so he ordered a starboard turn to initiate a circular manoeuvre. However, once complete, the manoeuvre did not result in the vessel gaining any distance. The pilot's expectation, combined with only using visual references, led to the vessel appearing to have gained a greater distance from the breakwater when in fact the distance remained the same. Then once the manoeuvre was complete, the pilot's attention was on getting the tugboats alongside the vessel and then slowing the vessel down in order to facilitate the starboard turn toward the pier.
1.9.2 Operational relationships between masters and pilots
In 1995, the TSB completed a safety study on the operational relationship between marine pilots and vessel masters or watchkeeping officers. The objective of this study was to identify safety deficiencies associated with teamwork on the bridge, including communication between marine pilots and masters or officers of the watch.
According to the study, when asked whether bridge officers are reluctant to question a pilot's decision, some 92% of masters and 81% of bridge officers stated that they were sometimes reluctant, and 11.5% of bridge officers replied that they were always reluctant to question the pilot's decisions. One master commented that, because the master is often on the bridge when a pilot has the con, bridge officers will hesitate to speak up because they rely on the master's experience and authority.Footnote 14
1.9.3 Pilot boarding procedures and continuous exchange of information
When a pilot boards a vessel, information is exchanged between the pilot, officer of the watch, and master. According to International Maritime Organization (IMO) Resolution A.960 (endorsed by the International Maritime Pilots Association), the exchange should include at a minimum information about intended courses and speed, areas to avoid, the vessel's manoeuvrability, and the pilot's intended approach. It is also important that both the vessel's passage plan and the pilot's passage plan are discussed during the initial master-pilot exchange, and that communication between the pilot and bridge team is continuous throughout the pilotage operation.Footnote 15
Sharing passage plans during the initial master-pilot exchange and throughout the pilotage operation enables pilots and all bridge team members to construct a shared mental model of how the voyage will progress.Footnote 16 IMO Resolution A.960 states that master/pilot “information exchange should be a continuous process that generally continues for the duration of the pilotage,”Footnote 17 especially because variables and discrepancies may affect the safe navigation of the vessel.
The Standards of Training, Certification and Watchkeeping for Seafarers Code (the STCW Code) also emphasizes the importance of an ongoing exchange of information between master and pilot, and states that “despite the duties and obligations of pilots, their presence on board does not relieve the master or officer in charge of the navigational watch from their duties and obligations for the safety of the ship.”Footnote 18
In the safety study conducted by the TSB in 1995, the Board noted that a pilot's decision making “can become the weak link in a system prone to single-point failure; i.e., in the absence of effective monitoring, there is little safety backup for the pilot in the navigation of the vessel.”Footnote 19 It is therefore important that the bridge team and pilot work cooperatively and share information to avoid a situation where single-point failure is possible.
In this occurrence, the SBI Carioca's Master/Pilot Information Exchange form was completed in accordance with the vessel's safety management system. The form contains a checklist with 13 items to be discussed among the bridge team: these include the roles and responsibilities of the master, the pilot, and other members of the bridge management team; the passage plan; and the berthing plan.
Although there was a brief exchange of basic vessel information (horsepower and stopping capability) between the master and the pilot, there was no exchange of passage plans or discussion of the above-noted items on the checklist. The pilot did not discuss with the master and the officer of the watch his intended circular manoeuvre to reposition the vessel for its approach to the Port of Belledune, and the master did not ask about the pilot's intentions.
Furthermore, the master did not communicate with the pilot the information that he was gathering from the ECDIS and radar, including courses, speed, and the rapidly approaching depth contour on which the vessel grounded. Information exchange throughout the pilotage operation was limited to the pilot's helm orders. The pilot did not request feedback from the bridge team, and none was offered.
1.10 Previous occurrences
The following previous occurrences involved vessel groundings in which information exchange was a factor.
M16C0005 (MSC Monica) – On 22 January 2016, the container vessel MSC Monica ran aground on the St. Lawrence River 1 nm north-northeast of Deschaillons-sur-Saint-Laurent, Quebec. The vessel sustained minor damage to the hull and major damage to its 4 propeller blades.
The Board determined that “[i]f bridge team members do not share a complete and common understanding of an emerging problem and continuously exchange information to solve problems, there is a risk that the bridge team's response will be premature, uncoordinated, and ineffective.”
M14C0193 (tug Vachon) – On 12 September 2014, the tug Vachon struck the breakwater in Port-Cartier, Quebec, while assisting the bulk carrier Orient Crusader to enter the harbour.
The Board determined that “[i]f bridge team members do not continue to actively participate in the monitoring of the vessel's progress when a pilot is on board, there is a risk that errors in navigation may go undetected.”
M14P0014 (Cap Blanche) – On 25 January 2014, the container vessel Cap Blanche grounded within the buoyed channel in the Steveston Bend, British Columbia. The vessel was under the conduct of a pilot and was in reduced visibility due to fog.
The Board determined that “[i]f information that may affect the safe passage of the vessel is not communicated between bridge teams and pilots, there is a risk that unsafe situations and conditions may persist.”
1.11 Active recommendations
On 08 May 1991, while downbound in the St. Lawrence River with a cargo of oil, the Canadian tanker Irving Nordic struck bottom to the north of the ship channel, downstream of Grondines wharf. The vessel exited the navigation channel in daylight and in good visibility. The Irving Nordic suffered considerable bottom damage. There were no injuries. Minor pollution was observed as the vessel arrived at Québec, Quebec, but the pollution was contained.
The Board determined that the Irving Nordic struck bottom because the vessel left the navigation channel as a result of a premature alteration of course.
The Board believes that close and continuous monitoring of a vessel's progress along the pre-planned track is essential for the safe conduct of the vessel. Knowledge of the pilot's passage plan would provide a focus for the officer of the watch to effectively monitor the intentions of the pilot, the track and the progress of the vessel. Currently, it is not common practice for pilots to provide passage plans to ship's personnel or for the pilotage authorities to provide such plans to their pilots. Therefore, in Marine Investigation Report M91L3012, the Board recommended that
the Department of Transport require that the pilotage authorities publish official passage plans for compulsory pilotage waters and make them available to masters to facilitate monitoring of the pilot's actions by the vessel's bridge team.
Transportation Safety Recommendation M94-34
In March 2017, the Board reassessed the APA's response to this recommendation. Although the APA did report to the TSB about related projects under its authority, it did not indicate that it was developing or publishing passage plans. Therefore, the Board's assessment of the APA's response is Unsatisfactory.
2.0 Analysis
The bulk carrier SBI Carioca, with a draft of 12.65 m, ran aground inside a 10 m depth contour located near the Port of Belledune, New Brunswick, as the pilot manoeuvred the vessel to establish an approach to the port's pier.
This analysis will focus on factors leading to the grounding, bridge resource management, pilot boarding stations, and configuration of the electronic chart display and information system (ECDIS).
2.1 Factors leading to the grounding
Because the vessel approached the pilot boarding station outside of the Belledune Port Authority's office hours, the SBI Carioca's crew could not obtain instructions from the port before the pilot boarded the vessel.
Nautical publications such as sailing directions contain multiple positions for the Port of Belledune's pilot boarding station. The station is not marked on any chart, whereas pilot stations are marked for other ports in the area.
When the pilot boat approached the SBI Carioca, the SBI Carioca's pilot ladder was dragging in the water and the crew had to raise it, delaying the pilot's boarding. By the time the pilot was on the SBI Carioca's bridge, the vessel was 0.9 nautical miles (nm) northeast off the pier, which left limited distance and time for a vessel of the SBI Carioca's size and manoeuvrability to make a safe approach to the pier.
When the pilot boarded the vessel, no information was exchanged between the pilot and the master relating to the pilot's intended manoeuvres.
The pilot's priority was to manoeuvre the vessel to gain greater distance from the pier and to reset the vessel's approach, while taking into account the time pressure associated with the imminent turning of the tide. He therefore ordered a starboard turn, engaging the vessel in a circular manoeuvre. Contrary to the pilot's expectation, the manoeuvre when completed did not result in the vessel gaining any distance from the pier.
The vessel's passage plan indicated a 14 m safety contour, but no alarm was set on the ECDIS. There was a lack of communication among members of the bridge team. The pilot positioned himself so that he had no visual access to the ECDIS or radar. As was his standard practice, he navigated the vessel by visual means. He did not request feedback from the bridge team on the progress of the vessel, such as the rate at which the vessel was advancing toward the 10 m depth contour. Similarly, the bridge team did not offer any feedback to the pilot. Without effective communication, there was no shared mental model among bridge team members. Additionally, because the ECDIS alarm had not been set, the pilot was not aware that the vessel had crossed the safety contour and was approaching the 10 m depth contour.
The expected outcome of the circular manoeuvre, combined with navigating using only visual references, led to the pilot's misperception that the vessel had gained more distance from shore than it actually did. Verification with electronic navigation displays is a defence against visual misperceptions.
Once the vessel completed its manoeuvre, the pilot's attention was focused on the vessel's speed and getting the tugs alongside the vessel. While the pilot was aware that the vessel was not heading towards the pier, he was not aware of its proximity to the 10 m depth contour, and the bridge team did not alert him to this hazard. Furthermore, a lack of situational awareness meant that the pilot did not realize the vessel was aground until about 9 minutes after the fact.
2.2 Bridge resource management
Continuous exchange of information and the establishment of clear roles for bridge team members are key components of BRM, and contribute to the safe navigation of the vessel.
The officer of the watch was not on the bridge, because he was raising flags on the mast atop the vessel's wheelhouse. The officer of the watch was therefore not a contributing member of the bridge team in the critical period leading up to the grounding.
Although the master and the pilot on board the SBI Carioca had received BRM training, in this occurrence, the bridge team did not apply the BRM principles of teamwork and open communication. As a result, the bridge team did not have a shared mental model from which to safely navigate the vessel.
The master was the only team member monitoring the ECDIS and the radars, while the pilot monitored the vessel's progress using only visual cues. The master did not communicate any information that he received from the ECDIS and the radars to the pilot, nor did the pilot request any. Therefore, as the vessel steadily progressed towards the 10 m depth contour where it grounded, the pilot was unaware that that the vessel was approaching the bank, and the vessel's speed was not sufficiently reduced.
According to the TSB's safety study on master/pilot exchanges conducted in 1995, passage plans, vessel characteristics, and local conditions are not communicated effectively between pilots and the ship's bridge team members. Even when watchkeeping officers are unsure of a pilot's intentions, many are reluctant to ask.
The study identified several possible reasons for the lack of communication:
- The belief on the part of many mariners surveyed that the handling characteristics of Canadian-registered ships are well known to pilots
- The possibility of pilots believing that Canadian officers are familiar with the routes and standard passage plans, so it is not necessary to discuss them
- Habit, or normal proceduresFootnote 20
Little information is routinely provided in the initial master/pilot exchange and throughout the passage, and there is little apparent demand for it. Neither pilots nor ship officers are expected to provide each other with much information, and so they do not.
As demonstrated by this occurrence and previous occurrences, shortcomings in the implementation of BRM principles have been a contributing factor in numerous marine accidents. If the principles of BRM are not used effectively, particularly with a pilot on board, bridge teams may be deprived of a shared mental model to safely navigate vessels.
2.3 Pilot boarding station
Vessels arriving at the Port of Belledune outside of business hours are unable to contact the port authority to finalize arrangements to bring the pilot on board. Both the Admiralty Sailing Directions and the Port of Belledune's publication that was sent to the master by the ship's agent provided contact information for the port. However, port offices were not open during the hours preceding the SBI Carioca's arrival, and the crew was therefore unable to clarify that the pilot's preferred location to board the vessel was 2 nm northeast of the pier.
It is critical that a deep-draft vessel arrive at pilot boarding stations with enough time to bring the pilot on board, conduct the pilot/master information exchange, and ensure that the vessel arrives at the pier before the turn of the tide. It is also critical to set the vessel's heading so that it can make a straight run at the pier and avoid excess manoeuvring: most conventional bulk carriers such as the SBI Carioca are not equipped with bow or stern thrusters and are typically driven by a single screw, limiting their manoeuvrability.
Without a symbol on the chart that clearly marked the location of the pilot boarding station, and with conflicting information regarding the station's exact location, the vessel was closer to the pier than was practical for a safe approach when the pilot arrived at the SBI Carioca.
In this occurrence, the delay in boarding resulting from repositioning the ladder meant that the pilot did not arrive on the bridge until 0655, when the vessel was 0.9 nm northeast of the pier and proceeding at a speed of 3.5 knots. After executing the circular manoeuvre, the vessel was still about 1 nm northeast of the pier, but was on a heading of 160° at a speed of about 6.5 knots. A normal course toward the pier would have been roughly southwest. Because the vessel did not advance as far to the northeast as the pilot had anticipated, this left the vessel no further away from the pier than it had been in before the manoeuvre and at a less favourable heading, and the pilot did not have sufficient time or distance to set up the approach as was intended.
Bringing a pilot on board without sufficient time to manoeuvre may be detrimental to a vessel's safe approach to a pier.
2.4 Passage planning
Passage plans contain key navigational elements such as the vessel's course, local hazards, visual cues and reference points, course alteration points, and wheel over positions.
The safety study conducted by the TSB in 1995 discusses the need for pilots to have a passage plan and share it with the master or officers of a vessel:
The Board is aware that, due to the dynamic nature of piloting a vessel, there will invariably be deviations from any detailed manoeuvring and passage plans. However, that is not to say that the pilot should not discuss with the master or [officer of the watch] his intentions for the conduct of the vessel. Such communication of intentions, be it in the form of a detailed or a general passage plan, could assist the [officer of the watch], particularly in restricted waters, to monitor and verify clearing bearings and radar safety ranges and contribute to the safety of the passage.Footnote 21
The pilot involved in this occurrence did not have a formal passage plan and did notshare his intentions with the master or other members of the bridge team either upon boarding or throughout the pilotage, aside from generally stating that the vessel was too close to the pier for a safe approach. The SBI Carioca's passage plan consisted of a single course from the pilot station to the pier.
If formal passage plans are not devised and shared among members of the bridge team, there is a risk that bridge team members will be unable to effectively monitor the pilot's actions with regard to the vessel's track and progress.
2.5 Configuration of the electronic chart display and information system
To ensure the safe passage of a vessel, navigators use visual cues and information from multiple types of navigational equipment and aids to navigation. This helps them maintain situational awareness with respect to the vessel's progress and allows for cross-checking to identify potential equipment or human errors.
The settings on the SBI Carioca's ECDIS can be adjusted by crew members to suit the navigator's purpose. One of these settings identifies depth contours of varying depths with shading. However, although a safety contour had been identified, no alarm had been set on the ECDIS.
In this occurrence, the shading was set to depict anything shallower than 20 m in dark blue, to differentiate it from deeper waters, which were identified with light blue. Had waters with a depth of 10 m and less been shaded with dark blue and marked distinctly as a no-go zone, the vessel's relatively rapid approach to the 10 m depth contour would have been more apparent, and it may have acted as a warning before the vessel went aground.
If settings, including alarms, on electronic navigation devices are not adjusted to emphasize identified hazards, those hazards may go unnoticed by the bridge team.
3.0 Findings
3.1 Findings as to causes and contributing factors
- Without a symbol on the chart that clearly marked the location of the pilot boarding station, and with conflicting information regarding the station's exact location, the vessel was closer to the pier than was practical for a safe approach when the pilot arrived at the SBI Carioca.
- Contrary to the pilot's expectation, the circular manoeuvre, when completed, did not result in the vessel gaining any distance from the pier.
- The pilot navigated the vessel by visual means and did not request or receive feedback on the vessel's progress from the bridge team. Without effective communication, there was no shared mental model among bridge team members.
- Because the alarm had not been set on the electronic chart display and information system, the pilot was not aware that the vessel had crossed the safety contour and was approaching the 10 m depth contour.
- The expected outcome of the circular manoeuvre, combined with navigating using only visual references, led to the pilot's misperception that the vessel had gained more distance from shore than it actually did.
3.2 Findings as to risk
- If the principles of bridge resource management are not used effectively, particularly with a pilot on board, bridge teams may be deprived of a shared mental model to safely navigate vessels.
- Bringing a pilot on board without sufficient time to manoeuvre may be detrimental to a vessel's safe approach to a pier.
- If formal passage plans are not devised and shared among members of the bridge team, there is a risk that bridge team members will be unable to effectively monitor the pilot's actions with regards to the vessel's track and progress.
- If settings, including alarms, on electronic navigation devices are not adjusted to emphasize identified hazards, those hazards may go unnoticed by the bridge team.
4.0 Safety action
4.1 Safety action taken
4.1.1 Atlantic Port Authority
At the request of the Atlantic Port Authority, a pilot boarding station symbol has been added to Canadian Hydrographic Services charts at 47°56′ N and 65°48′ W, approximately 2 nautical miles northeast of the Port of Belledune breakwater.
4.1.2 Transportation Safety Board of Canada
The Transportation Safety Board of Canada has sent marine safety advisories to the Canadian Department of Fisheries and Oceans and the United Kingdom Hydrographic Office to inform them of the addition of the pilot boarding station to the chart so that these organizations can update their respective sailing directions.
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Area of the occurrence