Loss of Control - Collision with Water
Seair Seaplanes Ltd.
de Havilland DHC-2 MK 1(Beaver) C-GTMC
Lyall Harbour, Saturna Island, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Seair Seaplanes Ltd. deHavilland DHC-2 MK 1 (serial number 1171, registration C-GTMC) was departing Lyall Harbour, Saturna Island, for the water aerodrome at the Vancouver International Airport, British Columbia. After an unsuccessful attempt at taking off downwind, the pilot took off into the wind towards Lyall Harbour. At approximately 1603 Pacific Standard Time, the aircraft became airborne, but remained below the surrounding terrain. The aircraft turned left, then descended and collided with the water. Persons nearby responded immediately; however, by the time they arrived at the aircraft, the cabin was below the surface of the water. There were 8 persons on board; the pilot and an adult passenger survived and suffered serious injuries. No signal from the emergency locator transmitter was heard.
© Minister of Public Works and Government Services Canada 2011
Cat. No. TU3-5/09-0397E
ISBN 978-1-100-18143-1
1.0 Factual Information
1.1 Flight Itinerary
The aircraft was on a multi-leg, visual flight rules flight from the water aerodrome at the Vancouver International Airport, British Columbia, to Mayne Island, Pender Island and Saturna Island and was returning to the Vancouver International Airport. Passengers and their baggage were to be picked up at every stop. The aircraft would be departing Saturna Island's Lyall Harbour with a full load of passengers. Before each departure, the pilot briefed the passengers about door locations, demonstrated the operation of the door opening handles, outlined the use of seatbelts as well as indicated the location of the life vests and the passenger safety briefing cards. There was no explicit briefing on how to egress the aircraft if submerged, nor was it required by regulation.
The aircraft was scheduled to depart from Lyall Harbour at 1600 Footnote 1 and sunset in Vancouver was at 1618. The normal flight time from Lyall Harbour to Vancouver is approximately 15 minutes. The aircraft would be required to land in Vancouver before the end of civil twilight, which was at 1654. Footnote 2
1.2 Weather
The 1600 aviation routine weather report for Victoria stated the following: wind 160° true at 13 knots, visibility 20 statute miles, few clouds at 800 feet above ground level (agl), few clouds at 1400 feet agl, 2500 feet agl and 5000 feet agl, a scattered layer of cloud at 20 000 feet agl, temperature 10°C, dew point 9°C and altimeter 30.24 inches of mercury.
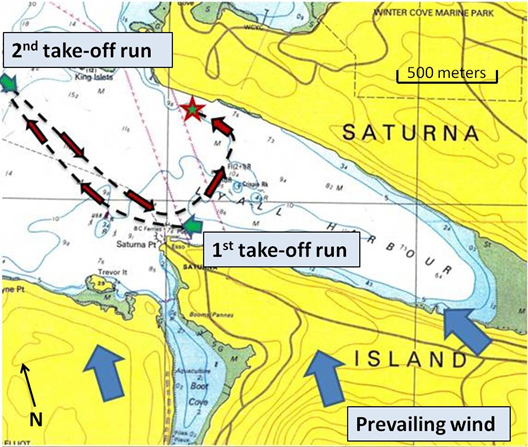
Around the time of the accident, the wind was of particular significance in Lyall Harbour. While local recordings showed the wind direction varying from 082° to 165° true, it was estimated to be generally from the southeast at 18 knots with gusts to 26 knots. With the winds from the southeast, the area used by floatplanes is in the lee of high terrain on the island (see Figure 1). These conditions are conducive to the creation of mechanical turbulence and mountain waves.
Mechanical turbulence results from wind flowing over or around terrain or obstructions. When the air near the surface of the earth flows over obstructions, such as bluffs, hills, mountains or buildings, the normal horizontal wind flow is disturbed and transforms into a complex pattern of eddies or irregular air movements. The strength and magnitude of mechanical turbulence depends on the wind speed, the terrain roughness (or nature of the obstruction), and the air stability. While the turbulence associated with a light wind may be negligible or light, when the wind blows faster and the obstructions are larger, the intensity of the mechanical turbulence increases and may extend to higher levels. Footnote 3
Mountain waves occur when: Footnote 4
- The wind direction is within 30° of the perpendicular to the ridge of high ground; and
- The wind speed at the crest of the ridge is 15 knots or greater.
Generally, the wind flows up the windward slope of rising terrain and, once passed the ridge, flows in a wave pattern. The wavelength and amplitude of the oscillations depend, in part, on the height of the ground, wind speed and atmospheric stability. Vertical currents within the oscillations of a wave can reach 2000 feet per minute.
A mountain wave can produce an area of turbulence in the lee and below the ridge. An area of lower pressure is created by the Bernoulli Effect Footnote 5 associated with the strong wind above the ridge. Contact with the earth's surface causes friction where the airflow then becomes rotary in nature. As with mechanical turbulence, the magnitude depends on the wind strength, nature of the terrain and air stability. If the air is moist, rotor clouds may form.
1.3 Pilot
The pilot held a commercial pilot license and was certified and qualified for the flight in accordance with existing regulations. The pilot had accumulated about 2800 hours total flight time, of which approximately 2350 were in the deHavilland DHC-2 (Beaver) aircraft. Most of the pilot's commercial experience was acquired on floatplanes, generally operating in the Gulf Islands, British Columbia.
The pilot had been off duty for 3 days prior to the accident and had flown 2.2 hours within the previous week. He had a restful sleep the night before. The pilot had not conducted any other flights prior to the occurrence flight. Fatigue was not considered an issue in this occurrence.
The pilot had received underwater emergency egress training 6 weeks prior to the accident. This training was not required by regulation, but the company arranged to have it offered.
1.4 Aircraft
Manufactured in 1957, the aircraft was configured with 4 doors: 2 forward doors, which provided access to the pilot and front passenger seats, and 2 main cabin doors. The main cabin door on the left side of the aircraft, located behind the pilot, is normally used for embarking and disembarking all passengers. The pilot normally closes and opens this door for the passengers. Pilots themselves use the left forward door. Once the main cabin doors are closed, the handle is not easily accessed by the person sitting next to it. When the door is closed, the handle is located aft of the centre seat. The right front and right main cabin doors are rarely used because they are usually located on the opposite (water) side when the aircraft is docked.
The occurrence aircraft originally served in the United States military during which time it was equipped with doors that could be jettisoned. The aircraft was first imported into Canada in the 1970s. As the jettisonable doors were not certified for civilian use in Canada, they were replaced with regular doors. There were no approved modifications to fit the aircraft with large breakable or jettisonable push-out style windows to augment emergency egress and none were fitted.
The following modifications had been completed by other owners before the aircraft was purchased by Seair Seaplanes Ltd. (Seair):
- Viking Air Limited Supplemental Type Certificate (STC) SA92-63: Modification to increase gross weight to 5500/5600 pounds; and
- Federal Aviation Administration (FAA) STC SA397NW: Gill type battery relocation from the aft fuselage to the forward face of the firewall.
As part of STC SA92-63, a stall warning system was installed, which consisted of a panel mounted light and a horn. The STC required that the stall warning system circuit be continuously powered, regardless of battery switch position. This is commonly referred to as a hot circuit. According to the STC, this was to be accomplished by connecting the stall warning system circuit to the cabin light circuit, which is protected by a 15-amp circuit breaker and is connected directly to the battery.
STC SA 397NW, which was designed to move the centre of gravity (CG) forward, required moving the battery from the tail section to the nose compartment of the aircraft. Part of this procedure involved removing the hot circuit and the 15-amp circuit breaker, originally intended for the cabin and anchor lights.
The modifications associated with STC SA92-63 and STC SA397NW were made by Victoria Air Maintenance. However, the related maintenance documentation could not be located by the previous owner. At some point, which could not be determined, the stall warning hot circuit was reconnected to the battery via a 5-amp fuse, instead of the original 15-amp circuit breaker. A 5-amp fuse would provide adequate protection for the 5-amp stall warning system.
The aircraft was sold to a company in the United States before it returned to Canada a second time, when it was purchased by Seair. During this import, a review of the aircraft's airworthiness did not identify any stall warning wiring issues. Furthermore, according to the maintenance procedures and the aircraft flight manual supplement, no checks were performed to confirm the stall warning system was serviceable.
While being operated by Seair, an emergency locator transmitter (ELT) test light (1-amp) and pilot map reading lights (5-amps) were added to the same hot circuit as the stall warning system (5 amps). Any 2 of these 3 systems operating at the same time could draw loads exceeding the 5-amp fuse, which could have caused the fuse to burn out.
At some point, the horn in the occurrence aircraft was modified to be less noisy by filling it with silicone sealant. This was not, however, documented. It should also be noted that if a horn is modified to reduce its noise level, it may not be heard over the noise produced by the engine at takeoff power.
1.5 Weight and Balance
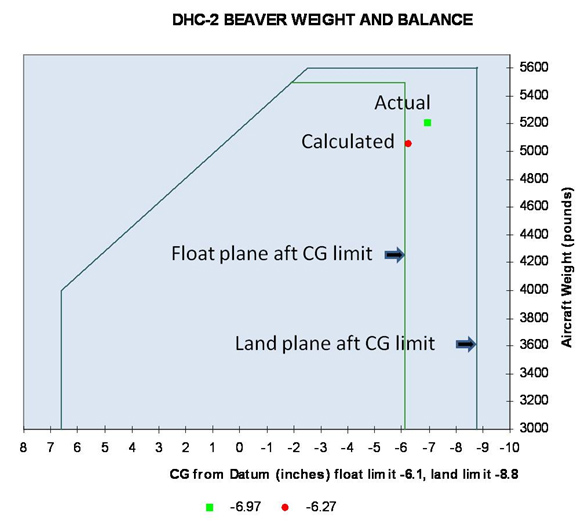
Circular slide rules were available on each aircraft for pilots to calculate the aircraft's weight and balance. The pilot calculated the takeoff weight as 5050 pounds with the CG at the floatplane aft CG limit (see Appendix A). These calculations were based on standard summer weights for the persons onboard; the baggage was estimated at 176 pounds.
Using the same data, TSB investigators initially calculated the CG to be at -6.27 inches (shown in red in Appendix A). The baggage was then dried and was found to weigh 214 pounds. Footnote 6 The aircraft's actual weight and balance at the time of takeoff was 5204 pounds (296 pounds below the maximum gross takeoff weight) and -6.97 inches (0.87 inches aft of the aft CG limit and shown in green in Appendix A).
1.6 Accident Sequence
Floatplane pilots departing Lyall Harbour typically take off in a westerly to northwesterly direction, which offers an unobstructed flight path and a more favourable route to Vancouver. After unsuccessfully trying to take off in a northwesterly direction (downwind), the pilot turned the aircraft into the wind and took off towards Lyall Harbour (see Figure 1).
The aircraft flight manual indicates takeoff flaps are to be used for takeoff. The flaps were set in the landing configuration for takeoff. Nothing in the aircraft flight manual prohibits a takeoff with flaps in this configuration.
After takeoff, the aircraft initially climbed and the pilot set the climb power. The flap position was not changed after takeoff. As the aircraft entered the harbour, the rate of climb decreased and the aircraft remained below the surrounding terrain. The pilot was concentrating on obtaining the best climb angle to clear the terrain and was looking outside. With the wind drifting the aircraft towards the northern ridge, the pilot turned the aircraft to the left (downwind) to leave the harbour.
During the turn, the left wing dropped, the nose pitched down and the pilot applied maximum power. The aircraft, however, descended rapidly. The stall Footnote 7 warning horn and the warning light were not detected at any point during the takeoff or upset. Just before impact with the water, the aircraft recovered to a wings-level and a slight nose-up attitude. However, the aircraft's descent rate remained high. Upon contact with the water, the floats collapsed upward into the wings and propeller. The pilot's seat failed and he was unrestrained, which likely contributed to the seriousness of his injuries and limited his ability to provide assistance to the passengers.
1.7 Wreckage Examination
Rescue divers found the aircraft in 14 meters of water in a nose-down, tail-up position. The right cabin and left cockpit doors were both open. The right cockpit and left cabin doors could not be opened.
The wreckage was recovered and transported to the TSB Wreckage Examination facility in Richmond, British Columbia. Damage was consistent with high energy impact at a flat attitude and high engine power.
The flight control mechanisms showed no evidence of pre-impact damage. The flaps were found in the landing configuration. A broken flap control rod left scars consistent with the flaps being at the landing setting at impact. The elevator trim was set close to full nose down trim.
The mixture was at idle cut-off and the throttle was at idle. Linkages to both these controls were broken.
The fuselage was deformed due to impact forces. As a result, the left cabin door, normally used for embarking and disembarking passengers, was jammed closed. The right cockpit door could only be opened with force.
There were 7 life vests on board: 5 were found in their storage pouches under the seats and 2 were free from their pouches. It could not be determined if these 2 had been removed by any of the passengers or if they had come free during the accident sequence or wreckage recovery.
The right cabin door window was broken, as was the window located over the baggage door. This allowed air to vent out and water to flow in following impact.
The pilot's seat frame remained attached to the floor, but the seat-back portion, including the lap belt attachments, had broken away. The front right seat (cockpit) did not fail.
The cabin light circuit breaker was tie-wrapped in the pulled position for undetermined reasons.
The following anomalies in the stall warning system were found:
- The horn had been filled with silicone;
- The filament in the light bulb for the stall warning system had not stretched, indicating that the bulb had not illuminated;
- The original hot circuit, with a 15-amp circuit breaker, had been removed;
- A new hot circuit had been installed with a 5-amp fuse;
- The map light and ELT had been added to the stall warning hot circuit; and
- The 5-amp fuse had burnt out.
1.8 Survival Aspects
The pilot was unconscious for a short time after impact. Upon regaining consciousness, the pilot escaped from the submerged cockpit, using his recent underwater egress training. The pilot exited through the pilot door on the left side, which had become unlatched at impact. The pilot then attempted to open the left main cabin door, but was unsuccessful. The pilot proceeded to the rear of the aircraft. The window over the baggage area was broken. The pilot reached in, but found no one. The pilot did not retrieve any of the life vests from the aircraft.
A passenger, who remained conscious throughout the incident, was seated in the centre row, next to the right cabin door. After undoing the seatbelt, the passenger floated away from the exit, into a bubble of air at the rear of the aircraft. Subsequently, the passenger was able to locate the right cabin door and escape. Upon exiting the aircraft, the passenger did not retrieve any of the life vests, but found 2 boat bumpers Footnote 8 at the surface that could be grasped. The passenger gave 1 of the bumpers to the pilot.
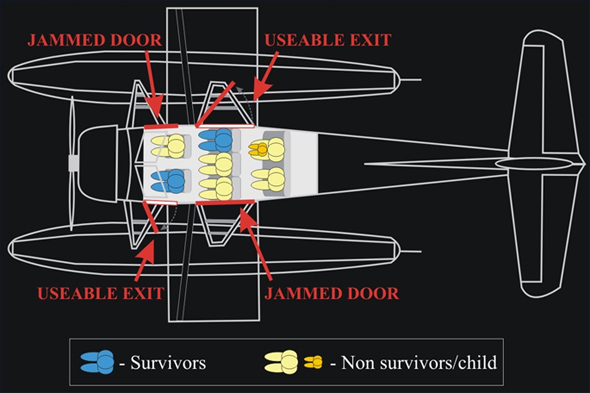
Four adult passengers had their seat belts undone. They were unable to exit the aircraft and drowned. The seating configuration is shown in Figure 2, which also indicates the useable and jammed doors.
Much of the impact force was absorbed by the floats and the fuselage. The g-force experienced by the individuals varied in relation to the force applied to the fuselage in the area where they were seated. The impact forces experienced by all onboard were considered survivable. Nevertheless, 6 passengers perished; only the pilot and 1 passenger survived the accident.
According to past research into accidents with aircraft submerged in water, typically only 10% to 15% of people are able to carry out the required egress actions effectively. Footnote 9 Another 10% to 15% of people typically fail to act from the extreme stress, greatly reducing their chance of survival. The remaining 75% may be stunned or shocked by the event; however, most are able to escape successfully if they are well trained and have rehearsed for such an event. Restrictions to normal exits, water temperature, darkness and disorientation following water impact further reduce the ability to egress. Escape training and passenger briefings emphasize the importance of memorizing exit locations. They are clearly identified in the passenger briefing cards; however, anecdotal information suggests few passengers refer to them.
Research has also shown that the ability to hold one's breath is a key factor in surviving an accident into water. Researchers have concluded that the inability to breath-hold has resulted in the 15% to 50% fatality rate in accidents into water. Footnote 10 One study indicated that the median breath-holding time of participants immersed in 25°C water was 37 seconds, which dropped dramatically between approximately 5 to 10 seconds in near freezing water temperatures. Footnote 11 In November, the average temperature of the water in this area is approximately 10°C. The use of an underwater breathing apparatus by properly trained occupants can extend the time available to egress a submerged aircraft.
If an individual is successful in escaping an aircraft that has impacted deep water, continued survival is a significant concern. The TSB Safety Study on Survivability in Seaplane Accidents (SA9401) suggests it is unlikely that persons faced with the urgency of escape in water will retrieve the life vests stored in the aircraft. Without a life vest, considerable amounts of energy are expended to remain above the surface. This physical effort can result in the loss of body heat, fatigue and eventual drowning. Survival without a life vest is further complicated by injuries.
1.9 Aerodynamic Stall
An aerodynamic stall occurs when the wing's angle of attack exceeds the critical angle at which the airflow begins to separate. When a wing stalls, the airflow breaks away from the upper surface and the amount of lift will be reduced to below that needed to keep the wing flying. While stalls occur at a given angle of attack, they can happen at any speed.
Airspeed is often used to predict stall conditions. The faster an airplane flies, the less angle of attack it needs to produce lift equal to weight. As the airplane slows down, the angle of attack needs to be increased to create the lift equal to weight. If an aircraft were to slow further, the angle of attack will be equal to the critical (stall) angle of attack at some point. Stall speed is the speed below which the airplane cannot create enough lift to sustain its weight in flight.
The speed at which a stall occurs depends on a number of things, such as the load factor, the manoeuvres being performed and gusts.
The load factor is the ratio of the lift of an aircraft to its weight and represents a measure of the stress, or load, to which the structure of the aircraft is subjected. The load factor is expressed in g, because of the perceived acceleration of gravity as felt by persons in an aircraft.
In straight and level flight, lift is equal to weight and the load factor is 1 (or 1 g). In a banked level turn, however, greater lift is required. This can be achieved, in part, by increasing the angle of attack (by pulling on the elevator control). Increasing the angle of attack increases the load factor. As the bank angle increases, there is a corresponding increase in load factor, which causes an increase in stall speed. As a result, the manoeuvre is often accomplished with the addition of power in order to maintain airspeed.
Gusts impose momentary increases in load factor. At the extreme, a gust, especially a vertical gust, can be strong enough to stall a wing.
The typical recovery from a stall initially involves levelling the wings, pushing the yoke forward (elevator down) and applying full or partial power. When the aircraft exhibits the first signs of recovery, a pilot gradually releases the nose down pressure. As the recovery progresses and flight is regained, pressure transitions to nose up (elevator up) with a view to recapturing lost altitude.
1.10 Stall Characteristics of the DHC-2
In 1947, the Beaver was certified to British Civil Airworthiness Requirements and its stall characteristics were found to be acceptable. However, the Beaver demonstrates little or no pre-stall buffet and, if a warning system is not installed, the onset of the stall may surprise pilots.
Test flights conducted in 1992 showed that the float-equipped Beaver (aft CG limit, wings level and at maximum continuous power) stalled at 55 mph indicated airspeed (IAS) with flaps in the takeoff setting and at 54 mph IAS with flaps in the landing setting.
Turn stall tests were not performed with a float-equipped Beaver. When a wheel-equipped aircraft was stalled at a 30° bank angle, it pitched nose down and rolled both into and out of the turn. The maximum roll was 50°. The maximum altitude loss was 100 feet before a pilot, using the proper technique, regained controlled flight. The test pilot noted that the Beaver displayed little or no pre-stall warning buffet.
Certification flight tests are conducted under controlled conditions. Under less than ideal conditions, like wind turbulence and unintended sideslip, stall characteristics could be aggravated with larger roll angles and increased altitude loss. Additionally, when an aircraft is unintentionally stalled, a pilot may not immediately recognize the condition and altitude losses in excess of 100 feet could be expected.
Some of the effects of an aft CG include:
- decreased stall speed of an aircraft;
- decreased longitudinal stability;
- violent stall characteristics; and
- poor stall recovery. Footnote 12
A 2009 FAA memorandum described the stall characteristics of the Beaver with a forward CG as being docile and predictable. However, many approved modifications have been applied to increase payload and make it easier to load to the aft CG limits. The FAA suggests the Beaver's stall characteristics in an aft CG condition are unstable and unpredictable, and that flight excursions with an aft CG are often unrecoverable at low altitude.
1.11 Post-accident Test Flights
Following the accident, test flights were conducted by Viking Air Limited under a Transport Canada (TC) issued flight permit. A Beaver similar to the occurrence aircraft was used to determine the aircraft's takeoff and climb performance with takeoff and landing flap. It was loaded to 5280 pounds and at the aft CG limit.
Takeoff test results showed that the aircraft would become airborne and reach 50 feet in 35 seconds with takeoff flap and 36 seconds with landing flap. The optimum climb gradient (angle of climb) was also remarkably similar. Both rates of climb at the test day temperature of 4°C to 5°C averaged approximately 500 feet per minute.
The best angle of climb speed is normally used to clear obstacles and these aircraft achieve that at 1.2 stall speed (v/vs) or 70 mph IAS with takeoff flap and 68 mph IAS with landing flap. During the test flights, the stall warning intermittently turned on and off at 1.1 v/vs.
1.12 Company Flight Operations
Seair pilots could obtain weather information through their dispatch located at the Vancouver International Airport. All company pilots are required to undergo a route check before operating at any of the company's normal destinations. Pilots are not required to contact dispatch on approach and departure. Passenger load is not always known by the company dispatch.
Following a 2004 occurrence, Footnote 13 the TSB issued Recommendation A04-01 which specifically called for the use of actual weights in performance calculations:
The Department of Transport require that actual passenger weights be used for aircraft involved in commercial or air taxi operations with a capacity of nine passengers or fewer.
This recommendation has not been fully implemented. In a 2008 update, TC indicated that Commercial and Business Aviation Advisory Circular 0235 and Policy Letter 168 had been issued to remind air operators that they are responsible for the accuracy of "…weight of passengers, carry-on baggage and checked baggage, determined either by actual weight, by using approved standard weights or by using approved survey weights, and the actual weight of cargo." TC also indicated that it had begun working on a Notice of Proposed Amendment, which will require affected air operators to use either actual passenger weights or segmented weight values derived from acceptable Canadian data sources, similar to Table 2-5 of FAA AC 120-27E, Aircraft Weight and Balance Control.
At Seair's main base of operation in Richmond, British Columbia, all of the passengers' baggage is weighed before loading. There were not, however, any scales at remote pick up sites. For weight and balance purposes, Seair periodically weighed passengers to establish average passenger weights. This process was documented in the company's operations manuals and approved by TC.
1.13 Previous Examination of Floatplane/Seaplane Safety
Over the past several years, the TSB has cited the increased risks of stalling associated with some aircraft types, in addition to the risks of drowning associated with egress following an impact with the water. In an effort to improve safety, the TSB has produced safety studies and safety advisories (Appendix B), as well as numerous aircraft accident investigation reports (Appendix C), which highlight issues related to floatplane/seaplane safety. This work discussed the benefits of wearing personal flotation devices and explicit egress briefings for passengers. It also described means to facilitate emergency egress, including quick release mechanisms and pop-out windows.
In addition to the above mentioned efforts, TC conducted a Floatplane Safety Review in 2005. Following this safety review, an internal report was produced, which recommended wearing life vests during takeoff and landing, offering enhanced flight crew training on submerged egress issues and improving emergency exit design. A public report was never released and this review did not result in any substantive change to existing regulations.
The TSB has found that the risk of drowning for occupants of seaplane accidents is high. The TSB and British Columbia's Coroners Service data show that, over the last 20 years, about 70% of the fatalities in aircraft that crashed and submerged in water were from drowning. In many cases, the deceased were found in the submerged wreckage.
Seaplane travel is common in Canada, particularly in provinces such as British Columbia where the only rapid means of travel is often by seaplane or helicopter. In the Vancouver Harbour alone, there are about 33 000 floatplane movements per year, carrying about 300 000 passengers.
2.0 Analysis
Except for the unserviceable stall warning system, examination of the wreckage revealed no pre-existing mechanical conditions that would have contributed to the accident. The following analysis focuses on the prevailing conditions, aerodynamic stalls and factors that led to this accident. In addition, it will elaborate on safety issues related to the broader subject of floatplane crash survivability in water.
The DHC-2 Beaver was originally certified without a stall warning system. One had been installed on the occurrence aircraft, as per the modification to increase gross weight STC. This system was, however, later rendered unserviceable. The absence of a functioning stall warning system, coupled with the known benign stalling characteristics of the Beaver, precluded any warning of an impending stall. Furthermore, the stall warning horn had been filled with silicone to make it less noisy. It is, therefore, possible that a horn may not be heard during periods of loud engine noise, thereby increasing the risk of inadvertent stalls.
The conditions in Lyall Harbour at the time of the occurrence were conducive to the development of mechanical turbulence and mountain waves. The turbulence associated with these phenomena likely contributed to vertical gusts, which subjected the aircraft to temporary, but significant increases in aerodynamic load.
Following takeoff, after the initial climb, the pilot commenced a left turn out of the harbour. The aircraft encountered down flowing air, restricting its ability to gain altitude. As the aircraft turned, it drifted towards terrain, causing the pilot to increase the bank angle. To maintain altitude while banking, the pilot likely had to increase the angle of attack, thereby increasing the load factor and the speed at which the aircraft would stall. While the use of flap may have increased the wing area and consequently decreased its loading, it was likely insufficient to counteract the combined loads brought about by the atmospheric conditions and increase in bank.
A float-equipped Beaver with the flaps set in the landing position was demonstrated to stall in straight and level flight at 54 mph. In this occurrence, the combined effects of the reduced airspeed during the climb, the bank angle during the turn and the atmospheric conditions increased the load factor of the aircraft to the point of aerodynamic stall.
The aircraft was under its maximum gross takeoff weight, but loaded such that its CG was beyond the aft limit for floatplane operations. The aircraft levelled off prior to impact, indicating the pilot had initiated stall recovery. Full recovery was compromised by the aft CG. Controllability notwithstanding, the altitude from which recovery was made was insufficient to arrest the descent, causing the aircraft to strike the water.
The damage to the pilot's seat rendered the restraint system ineffective and contributed to the pilot's injuries. These injuries, which included a brief loss of consciousness, caused a delay in the pilot's egress and limited his ability to provide assistance to the passengers.
With the exception of one adult, all passengers undid their seatbelts, indicating that they likely remained conscious after impact. Following the impact, the passengers would have had a few seconds to locate a suitable egress point, release their seat belts and exit the aircraft.
In this occurrence, the aircraft was not equipped with jettisonable doors or windows. As a result, the only possible egress points were the 4 doors on the aircraft. However, impact damage jammed 2 of the 4 doors and restricted egress from the sinking aircraft, which meant all 7 passengers and the pilot would have had to exit via 1 of 2 usable egress points. Rather than deliberately attempting to open a door, the surviving passenger exited through the door that had opened as a result of impact forces. It is likely that the pilot's recent egress training contributed to him being able to open the door and escape from the aircraft. The lack of alternate emergency exits, such as jettisonable windows, increases the risk that passengers and pilots will be unable to escape a submerged aircraft due to structural damage to primary exits following an impact with the water.
Seeing as the impact forces experienced by all onboard were considered survivable, the issue of timely escape contributed to the passengers drowning. Many persons could improve their chances of survival by identifying the possible exits and mentally rehearsing their actions, including identifying alternate exits in the event of an accident. If passengers are not provided with explicit safety briefings on how to egress the aircraft when submerged, there is increased risk that they will be unable to escape following an impact with the water.
Given the time involved in conducting a rescue, in cases when an individual is successful in escaping an aircraft following an impact, continued survival is a significant concern. This is particularly true if the individual has been injured. Since it is unlikely that persons faced with the urgency of escape in water will retrieve life vests stored in the aircraft, passengers and pilots not equipped with some type of flotation device prior to an impact with the water are at increased risk of drowning once they have escaped the aircraft.
3.0 Findings
3.1 Findings as to Causes and Contributing Factors
- The combined effects of the atmospheric conditions and bank angle increased the load factor, causing an aerodynamic stall.
- Due to the absence of a functioning stall warning system, in addition to the benign stalling characteristics of the Beaver, the pilot was not warned of the impending stall.
- Because the aircraft was loaded in a manner that exceeded the aft CG limit, full stall recovery was compromised.
- The altitude from which recovery was attempted was insufficient to arrest descent, causing the aircraft to strike the water.
- Impact damage jammed 2 of the 4 doors, restricting egress from the sinking aircraft.
- The pilot's seat failed and he was unrestrained, contributing to the seriousness of his injuries and limiting his ability to assist passengers.
3.2 Findings as to Risk
- There is a risk that pilots will inadvertently stall aircraft if the stall warning system is unserviceable or if the audio warnings have been modified to reduce noise levels.
- Pilots who do not undergo underwater egress training are at greater risk of not escaping submerged aircraft.
- The lack of alternate emergency exits, such as jettisonable windows, increases the risk that passengers and pilots will be unable to escape a submerged aircraft due to structural damage to primary exits following an impact with the water.
- If passengers are not provided with explicit safety briefings on how to egress the aircraft when submerged, there is increased risk that they will be unable to escape following an impact with the water.
- Passengers and pilots not wearing some type of flotation device prior to an impact with the water are at increased risk of drowning once they have escaped the aircraft.
4.0 Safety Action
4.1 Action Taken
4.1.1 Seair Seaplanes Ltd.
Seair has equipped each aircraft with hand-held baggage scales to allow pilots to make more accurate weight and balance calculations.
Seair has ordered new door latch release and window modification kits from Viking Air Limited.
Seair has enhanced its pre-flight safety briefing by now including an independent demonstration of where to find the life vests, what they look like and how to put them on. A mannequin located at the Vancouver and Nanaimo Seair docks is used to perform this safety demonstration. Enlarged photographs from the safety briefing cards are displayed on the mannequin stand. A briefing is provided to passengers before they head down to the aircraft at the dock and a second safety briefing is provided once they are at the aircraft.
4.1.2 Viking Air Limited
Viking Air Limited, the aircraft type certificate holder, has made push-out window and cabin and cockpit door latch kits available for installation on Beaver aircraft.
4.1.3 Transport Canada
Since this accident, the Board is encouraged to note that Transport Canada has completed a number of initiatives including:
- publishing articles in the Aviation Safety Letter to promote egress training and effective passenger briefings;
- developing posters and pamphlets for distribution to floatplane passengers to increase awareness of their role in safety;
- tasking its inspectors to ensure floatplane operators receive the latest safety promotion materials, to emphasize the importance of egress training and better passenger briefings during their visits and to conduct follow-up telephone surveys of floatplane operators to verify that they are using the safety promotion materials;
- developing a web portal to centralize floatplane safety information for use by operators and passengers and encouraging floatplane operators to provide a link to the portal from their websites;
- producing a video for use by operators promoting best practices and lessons learned in floatplane operations;
- producing a video for use by floatplane passengers on their role in safety; and
- facilitating a meeting of floatplane operators in October 2010, which resulted in the formation of an industry–led safety association of B.C. floatplane operators.
4.2 Safety Action Required
4.2.1 Emergency Egress for Seaplanes
Seaplane travel is common in Canada, particularly in provinces such as British Columbia where the only rapid means of travel is often by seaplane or helicopter. In the Vancouver Harbour alone, there are about 33 000 floatplane movements per year, carrying approximately 300 000 passengers.
The TSB has found that the risk of drowning for occupants of seaplane accidents is high. The TSB and British Columbia's Coroners Service data show that, over the last 20 years, about 70% of the fatalities in aircraft that crashed and submerged in water were from drowning. Half of the deceased were found in the submerged wreckage. While it could not be determined in all cases, some investigations found that the occupants were conscious and able to move around the cabin before they drowned. These past occurrences validate the probability that able bodied persons can be trapped in sinking aircraft and drown as a result.
This investigation concluded that some passengers survived the impact, but drowned because 2 of its 4 normal exits jammed shut. Had all normal exits been usable or had there been other emergency exits, such as jettisonable windows, there would have been a greater probability of escape from the aircraft and a greater chance of surviving the accident. Optional jettisonable windows for the DHC-2 model have been developed, but this only addresses 1 of the many aircraft types operated from water. Furthermore, there is no regulatory requirement for the installation of such emergency exits. Therefore, the Board recommends that:
The Department of Transport require that all new and existing commercial seaplanes be fitted with regular and emergency exits that allow rapid egress following a survivable collision with water.
A11-05
4.2.2 Wearing of Personal Flotation Devices
In many accidents when occupants escape from sinking aircraft, they egress without life vests, which may result in drowning. It has been shown that those inside a sinking aircraft understandably focus on escaping from it. In their haste to escape, occupants either do not often have enough time to locate and don a life vest or they overlook doing so. In this accident, 2 of the seriously injured occupants were able to escape from the aircraft, but neither person, including the pilot who had been trained for underwater egress, managed to retrieve a life vest from the aircraft. Had they not used nearby boat bumpers to stay afloat, they could easily have drowned.
Some operators, notably Transport Canada with its fleet of aircraft, require those in aircraft taking off or landing on water to wear approved life vests. Such a requirement eliminates the need for occupants to search for their life vest and, after they escape from the aircraft, the life vest is ready for use. Without a personal flotation device, and in the absence of other rescue capabilities, there is higher risk that survivors of water impact would drown.
The TSB has previously recommended (A94-07) that seaplane occupants be required to wear personal flotation devices during flight. A number of objections to this solution have been raised by the regulator and industry, including emergency inflation before egress hampering the wearer and impeding the egress of others, sizing issues, especially over thick outer clothing, and discomfort. These objections may have some validity when considering traditional life vest models. Recent developments in personal flotation device design include such things as manually-inflated belt packs, which are donned only after inflation. When combined with an appropriate and well-understood passenger briefing, such devices would effectively counter those objections.
The evidence continues to support the conclusion that, unless persons don a personal flotation device, they are unlikely to use one after escaping an aircraft in water. Therefore, the Board recommends that:
The Department of Transport require that occupants of commercial seaplanes wear a device that provides personal flotation following emergency egress.
A11-06
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
5.0 Appendices
Appendix A – Weight and Balance Graph
Appendix B – TSB Safety Studies and Safety Communications Related to Floatplane / Seaplane Safety
-
A Safety Study of Piloting Skills, Abilities, and Knowledge in Seaplane Operations (TSB report SSA93001): This 1993 study examined 1432 seaplane accidents. Although the study did not focus on survivability issues, it did compare the ratio of fatal accidents to total accidents for float-equipped aircraft to that of wheel-equipped (for those makes and models of aircraft most frequently float-equipped). When these aeroplanes were on wheels, 10% of the accidents were fatal. However, when they were on floats, 17% were fatal. In the study, 10 safety recommendations were made aimed at reducing the number of seaplane accidents.
-
A Safety Study Of Survivability in Seaplane Accidents (TSB report SA9401): A 1994 TSB Safety Study analyzed seaplane accidents in Canada over the 15 year period from 1976 to 1990. During that time, there were 1432 such accidents, of which 234 resulted in 452 fatalities. The safety study contained 6 recommendations to enhance the survivability of persons involved in seaplane accidents, including a recommendation on wearing personal flotation devices during the standing, taxiing, takeoff, approach and landing phases of flight (TSB Recommendation A94-07).
-
TSB Safety Advisory A000003-1, Escape from a Submerged Seaplane: The TSB issued this safety advisory following an accident in 2000 involving a de Havilland DHC-2 Beaver. Amongst other things, the safety advisory suggested that quick release mechanisms or push-out windows would enhance rapid egress. Transport Canada did not, however, implement requirements for those modifications to floatplanes;
-
TSB Safety Advisory A040044-1, Egress from Submerged Seaplanes: The TSB issued this safety advisory following a 2004 accident involving a Cessna A185F seaplane carrying 1 pilot and 3 passengers. In this occurrence, the pilot and the right front-seat passenger were unable to open either of the main exits and egressed through the broken window in the left cabin door. Despite the 2 rear-seat passengers not sustaining any physical injuries during the occurrence, they drowned. The advisory stated that modifications to seaplane doors to provide a quick release mechanism, or the fitting of pop-out windows, would enhance the opportunity for rapid egress in the event that the aircraft becomes submerged. The advisory suggested that TC may wish to consider additional methods to facilitate rapid emergency egress from seaplanes in the event that the cabin becomes submerged. In its response, TC indicated that jettisonable doors or large frangible or pop-out windows that would facilitate emergency exits is within the authority of the state of design authority and that TC will not take any action relating to this issue.
-
TSB Aviation Safety Information Letter A040046, Passenger Briefings and Safety Features Cards in Seaplane Operations: This information letter was produced following the 2004 accident involving a Cessna A185F seaplane cited above in the previous paragraph. The information letter highlighted that the regulations were not instructive with regard to a requirement for the briefing to include information specific to underwater egress procedures in seaplane operations. Furthermore, there is no requirement for seaplane safety feature cards to contain information or special procedures unique to underwater egress. The information letter concluded by highlighting that the risks associated with seaplane passengers and pilots being trapped inside a submerged aircraft are increased when the pre-flight safety briefing and the safety features cards do not include information specific to underwater egress. In its response, TC advised that it sent 100 copies of its revised brochure entitled Seaplanes – A Passenger’s Guide (TP 12365) to every commercial seaplane operator in Canada, with instructions on how to order more if needed.
Appendix C – TSB Aircraft Accident Investigation Reports Citing Seaplane Egress Difficulties
| Occurrence | Type | Fatalities | Comments |
|---|---|---|---|
| A86P0058 | DHC-2 Beaver | 5 | The pilot escaped with serious injuries and 5 passengers drowned. The report highlighted that, with the centre seat installed, the rotary knob for opening the rear door is located behind the seat. As such, the door cannot easily be opened by passengers sitting in the centre seat. |
| A87P0021 | Cessna A185F | 1 | The pilot was unable to escape from the submerged aircraft and drowned. |
| A87P0901 | Cessna 180J | 1 | The pilot was able to escape from the submerged aircraft through the left-hand door. He then repeatedly dived underwater in an attempt to rescue his wife, but was unable to locate her. She was found by rescuers at the rear of the cabin 20 minutes later, but died in hospital several days after the accident. Neither occupant suffered incapacitating injuries during the crash sequence. |
| A88O0203 | DHC-2 Beaver | 2 | The pilot and front-seat passenger were unable to escape from the sinking aircraft and drowned. |
| A89C0089 | Cessna A185 | 1 | One of the four occupants was trapped in the aircraft and drowned. |
| A89O0369 | Cessna TU206G | 1 | The pilot exited the aircraft by kicking open the port door window. However, there was no door beside the front passenger; that passenger was unable to egress and drowned. |
| A90W0265 | DHC-2 Beaver | 2 | One passenger was able to egress; however, the pilot and second passenger did not and drowned. Damage to the wings blocked both right doors and the left cabin door. |
| A91C0122 | DHC-2 Beaver | 1 | The pilot survived the impact, but drowned while trying to escape from the wreckage. |
| A91Q0267 | Cessna A185F | 2 | The handle of the right door was broken, however, the passengers occupying the right front seat managed to exit the aircraft through the window of the right door. The pilot and rear seat passenger, who had no signs of physical trauma on their bodies, drowned. |
| A94O0213 | Cessna A185E | 3 | One passenger was able to exit the aircraft through the left door window and swim to shore. The pilot and other 2 passengers did not survive. Both doors remained closed throughout the impact, but both side door windows were fully open when the aircraft was located. |
| A96Q0114 | Cessna U206F | 4 | The pilot and 3 passengers drowned inside the aircraft. Prior to this occurrence, the Canadian Aviation Safety Board forwarded an Aviation Safety Advisory to Transport Canada indicating that the rear double cargo door of the Cessna 206 was hard to open. No measures were taken to have the doors modified. |
| A97C0090 | Cessna TU206G | 2 | The 2 passengers were unable to exit the aircraft and drowned. |
| A97P0230 | Cessna 180J | 3 | All 3 occupants drowned following a survivable impact with the water. |
| A98P0215 | DHC-2 Beaver | 5 | All 5 occupants drowned following a survivable impact with the water. Medical information revealed that the occupants had been restrained during the initial impact and rollover. |
| A00P0103 | DHC-2 Beaver | 3 | In this fatal occurrence, the aft CG contributed to the cause of the accident. This aircraft had no stall warning system. Two passengers were unable to escape the aircraft and another drowned while attempting to swim to shore. |
| A03Q0083 | Cessna U206F | 1 | The pilot exited and told the passenger to follow. The passenger, disoriented, went to the rear of the aircraft and drowned |
| A03F0164 | Cessna 185 | 1 | One passenger was unable to escape from the aircraft and drowned. |
| A04W0114 | Cessna 185F | 2 | The survivors were unable to locate the interior door handles after the seaplane became inverted and submerged in the water, thus preventing them from using the doors as emergency exits. The TSB report contained the following Board Concern: “Based on historical data, occupants of submerged seaplanes who survive the accident continue to be at risk of drowning inside the aircraft. Existing defences against drowning in such circumstances may not be adequate. In light of the potential loss of life associated with seaplane accidents on water, the TSB is concerned that seaplane occupants may not be adequately prepared to escape the aircraft after it becomes submerged. The Board is also concerned that seaplanes may not be optimally designed to allow easy occupant egress while under water.” |
| A05Q0178 | Cessna 185F | 1 | After the aircraft capsized while attempting to take off, 5 occupants were able to escape. One occupant, seated in the front right seat, was unable to escape the submerged cabin and drowned. |
| A05O0147 | Cessna 185F | 1 | In this occurrence, the pilot drowned. The Board signaled its concern as follows: “Based on historical data, occupants of submerged seaplanes who survive the accident continue to be at risk of drowning inside the aircraft. Existing defences against drowning in such circumstances may not be adequate. In light of the potential loss of life associated with seaplane accidents on water, the TSB is concerned that seaplane occupants may not be adequately prepared to escape the aircraft after it becomes submerged. Of equal concern is that the rescuers, in this occurrence, could not access the cabin from outside.” |
Appendix D – TSB Aircraft Accident Investigation Reports Citing Seaplane Centre of Gravity Issues
| Occurrence | Type | Fatalities | Comments |
|---|---|---|---|
| A98P0194 | DHC-2 Beaver | 0 | The TSB investigation reported on the poor stall characteristics of the aircraft with an aft CG loading. In this occurrence, the aircraft was not equipped with a stall warning system. |
| A00P0103 | DHC-2 Beaver | 3 | In this fatal occurrence, the aft CG contributed to the cause of accident. This aircraft had no stall warning system. Two passengers were unable to escape the aircraft and another drowned while attempting to swim to shore. |
| A01P0194 | DHC-2 Beaver | 5 | The investigation determined that exceeding the aft CG limit produced rapid and uncontrolled aircraft attitudes after a stall from which the pilot could not recover before striking trees. This aircraft had no stall warning system. |
| A03W0210 | Piper PA–18–150 | 2 | The aircraft stalled at low altitude, which precluded an effective recovery; the aircraft was not fitted with a stall warning system, which may have delayed the pilot’s recognition of the impending stall. In addition, it was determined that the aircraft was above the maximum allowable seaplane gross weight and that the aft CG limit had been exceeded, which would have adversely affected the pilot’s ability to recover from a stall condition. |