Main-rotor strike and collision with terrain
VIH Helicopters Ltd.
Bell 407 (Helicopter), C-GNVI
Stewart, British Columbia 14 nm N
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The VIH Helicopters Ltd. Bell 407 helicopter (registration C-GNVI, serial number 53847) departed Stewart Airport at about 0943 Pacific Daylight Time (PDT), with the pilot and 2 passengers on board. The helicopter flew to a geological exploration site 14 nautical miles north of Stewart, British Columbia, adjacent to the Nelson Glacier. There were no further voice communications with the occurrence aircraft following departure, and flight tracking data stopped at 1004 PDT. Approximately 6 hours later, the wreckage of C-GNVI was discovered strewn down the steep mountain side at the exploration site. There were no survivors. The 406-megahertz emergency locator transmitter had activated, but the antenna and antenna cable were damaged, and a signal was not received by the Canadian Mission Control Centre. There was no fire.
Factual information
History of the flight
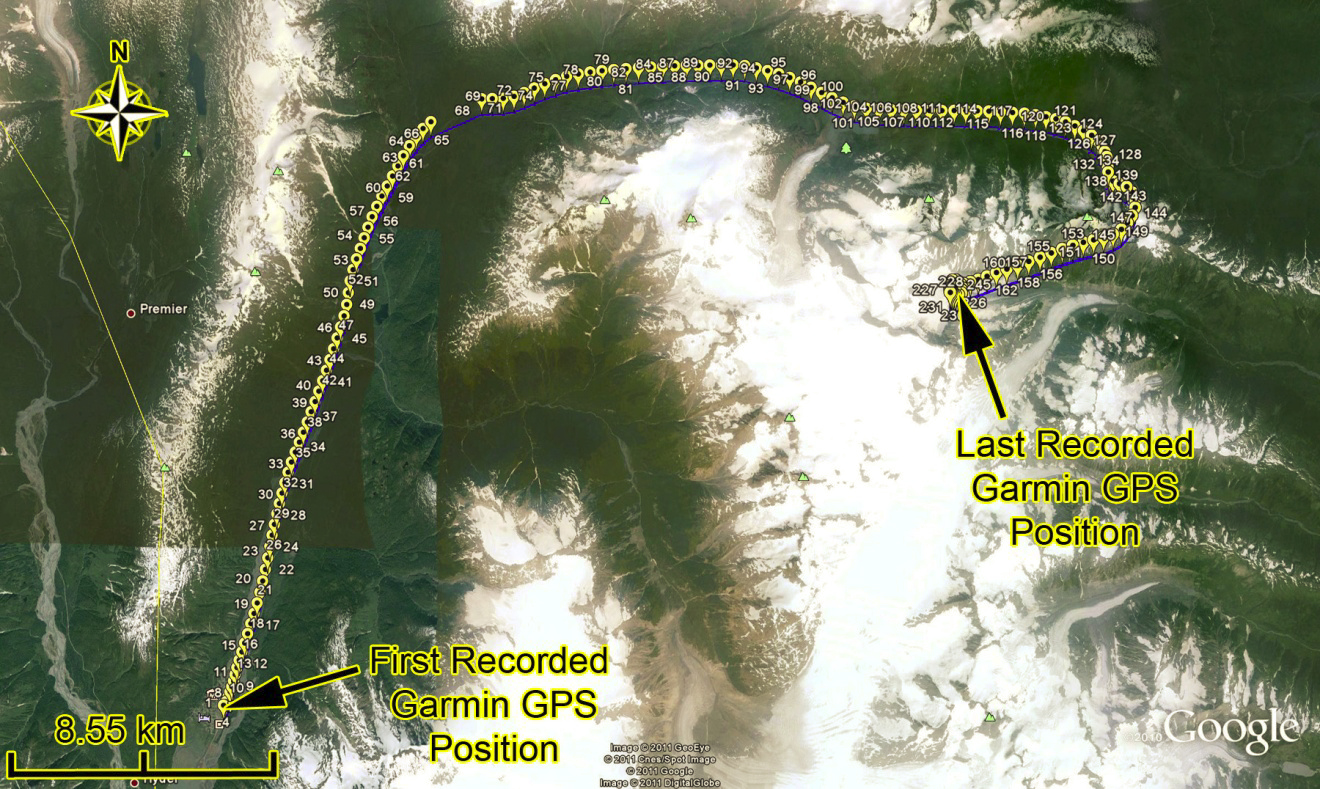
Using information retrieved from handheld cameras, a portable global positioning system (GPS), and an on-board GPS tracking system (which sends tracking information to the operator), the investigation determined that, at approximately 0958, Footnote 1 the occurrence helicopter performed a left-skid toe-in landing Footnote 2 on a mountain ledge at 5100 feet above sea level (asl). One passenger was seated in the left front seat adjacent to the pilot; the other was seated in the left rear forward-facing seat. The passengers had flown once before with this pilot. Both passengers were familiar with helicopter operations, and were proficient with hover-entry and -exit procedures. Footnote 3 The passenger in the rear seat performed a hover exit to retrieve a climbing rope that had been left behind the previous day. The other passenger remained on board. The helicopter lifted off and backed away to allow the passenger to retrieve the rope. The helicopter then landed a second time to pick up that passenger. This takeoff and subsequent landing were not reported by the GPS tracking system, as the reporting criteria were not met.Footnote 4 At 1001, the helicopter lifted off again, with both passengers on board. The GPS tracking system reported the take-off. The helicopter was manoeuvred slowly across the face of the mountain from left to right (when facing the mountain), circled to the left around the peak, and made another slow pass in the same direction across the mountain face. At 1004, the GPS tracking system reported that the occurrence helicopter had landed about 760 feet above the rope pick-up location. That was the last position and altitude reported by the GPS tracking system. At 1014, the GPS tracking system software generated an inactive status display, indicating that the system had not received a position report for 10 minutes.
Weather
The 1000 aviation routine hourly weather report for Stewart Airport reported the following: winds 230° true (T) at 5 knots; visibility 12 statute miles (sm), with a few clouds at 400 feet above ground level (agl), scattered at 1200 feet agl, broken at 5700 feet agl, and broken at 14 000 feet agl; temperature 12°C; dew point 11°C; altimeter setting 29.96 inches of mercury; and visibility lower to the north. Video footage filmed from the helicopter just before the accident depicted smooth flying conditions, broken mid-level cloud conditions with ragged ceilings, and good visibility below. Flagging tape at the climbing-rope pick-up site indicated near-zero wind conditions. Thin clouds surrounded some higher mountaintops. The weather was not considered to be a factor in this occurrence.
Flight Following
VIH Helicopters Ltd. conducts operations in accordance with Canadian Aviation Regulations (CARs) Part VII, Subparts 2, 3, and 4, and utilizes a Type D operational control system. Under this system, the pilot-in-command (PIC) is delegated authority over the initiation, diversion, and termination of flights with company aircraft. The company operations manual (COM) defines flight following as the monitoring of a flight's progress and the notification of authorities if the flight becomes overdue or goes missing. Current information on the location of company aircraft is required to be maintained at an appropriate location. For the occurrence flight, flight following was carried out from the Stewart base.
As per Section 3.2 of the COM, and in accordance with CARs 703.18, an operational flight plan is required for every flight. In addition, the COM states that pilots are required to advise flight-following personnel if they encounter unexpected delays that will cause them to return later than expected. On the day of the occurrence, the pilot's intentions for the day were verbally communicated by the pilot. Before the occurrence, the pilots and base personnel commonly relied on verbal operational flight plans. There was no written record of an operational flight plan for the occurrence flight. A wallboard at the Stewart base was available and designed for this purpose, but was not used. In addition, it was not common practice for pilots to specify a precise return time. This was largely due to the nature of the operation, which often required pilots to stay at an exploration site longer than expected when necessary to wait out weather, to relocate workers from the exploration group (referred to as climbers), or to sling equipment to climbers. On the day of the occurrence, the climbers' task for the day was to work from the current rappel to take rock samples from the cliff area of the work site. In addition, they were to check, from the helicopter, an area of interest to the climbers' right (west) of the current rappel. Before the helicopter's departure, ground personnel in Stewart received an indication from the pilot that, weather permitting, the pilot would be returning to Stewart after dropping off the climbers to make additional flights. The pilot did not specify a return time.
At the time of the occurrence, there was no established procedure at this base for using a time-based check-in call to report on personnel or helicopter status throughout a flight, nor was it common practice there. However, there are a number of repeater sites established throughout the area that are typically used by ground personnel to monitor aircraft activity. In many cases, ground personnel are able to keep track of the progress of aircraft in the area by listening to radio communications between operator aircraft and crews at work sites.
In addition to use of radio communications, the progress of flights can be monitored via an Internet web site, using the GPS tracking system installed on operator aircraft. The system reports its position at 2-minute intervals, as well as reporting landings and take-offs that meet the criteria established by the operator. The system also incorporates an emergency function that, if activated manually from the helicopter, increases the reporting frequency to 15 seconds and activates alarms through the monitoring notification system. The GPS tracking-system web site was monitored by personnel at the Stewart base periodically throughout the day of the occurrence. The tracking web site reported that the GPS tracker had gone inactive near the planned drop-off location. There was no indication that the emergency function had been activated. Since it was normal to receive the inactive message whenever a helicopter was shut down, ground personnel at Stewart assumed that the pilot had probably landed and shut down to wait out poor weather.
Overdue-aircraft Response
Ground personnel at Stewart expected the occurrence helicopter to return by approximately 1100. When the helicopter did not arrive as expected, ground personnel attempted to contact the helicopter via its VHF (very high frequency)−AM and VHF-FM radios. In addition, attempts were made to establish radio contact with the helicopter's occupants on personal VHF-FM radios that had been supplied to each of them. During the attempt to call the pilot's personal FM radio, it was discovered that the pilot's radio had been left in the hangar. The occurrence helicopter was not equipped with satellite communications. All attempts to contact the helicopter and its occupants proved unsuccessful. The exploration group had placed portable repeater stations on various mountaintops to extend communications between the base at Stewart and other exploration camps in the area. VHF radio signals travel on a line-of-sight basis. The location and terrain around the Nelson Glacier exploration project prevented line-of-sight communication between the helicopter and the nearest repeater from certain areas of the exploration site and from lower altitudes. When communications could not be established, and given the inactive status reported by the GPS tracking system, ground personnel believed that the occurrence helicopter had likely landed to wait for weather to improve before returning to Stewart.
By 1500, staff members of VIH Helicopters Ltd. and the exploration contractor decided to call in a helicopter from another site to investigate the status of C-GNVI, based on the last reported position of C-GNVI from the GPS tracking system. On board the search helicopter were 1 pilot and a maintenance engineer. They were not familiar with the site, and were unable to locate the helicopter or the climbers. In addition, attempts to establish radio communications with the occurrence helicopter or climbers were unsuccessful. The search helicopter then flew to a nearby staging area, and picked up first-aid equipment and 2 geologists with first-aid training. The geologists were familiar with the site, and were able to quickly locate the wreckage. Shortly thereafter, it was determined that all 3 persons on board C-GNVI had sustained fatal injuries.
The COM includes an overdue-aircraft response plan. As part of that plan, the operator will conduct a flight-route check. The procedure also states that the Joint Rescue Coordination Centre (JRCC) shall be contacted to confirm whether an emergency locator transmitter (ELT) signal has been received, and to alert the JRCC that search-and-rescue (SAR) services may be required. The JRCC was not notified that the occurrence aircraft was overdue and that the operator had commenced an air search. At that point, ground personnel believed that they would have been contacted by JRCC if an ELT signal had been received.
Aircraft
The Bell 407 is a single-engine, 7-seat, single-pilot, turbine-powered helicopter. It has a 4-blade main rotor. The pilot flies from the right-hand seat. C-GNVI was equipped with a high-mount external cargo basket installed on the right-hand side of the helicopter. Passengers normally embarked and disembarked through the left-side passenger doors. The flight controls for the left-hand pilot seat had been removed, and the cyclic and collective stubs were protected by semi-rigid covers.
The engine incorporates a full-authority digital electronic control (FADEC) system, which is comprised of 2 main units: an electronic control unit (ECU) and a hydro-mechanical unit (HMU). The ECU monitors and/or controls engine operating parameters related to
- speeds (main rotor, gas turbine, and power turbine revolutions per minute [rpm]);
- engine control inputs (power-lever angle on the fuel control unit, torque, and collective pitch angle);
- temperatures (measured gas temperature and compressor-inlet air temperature);
- fuel flow (pounds per hour); and
- ambient air pressure.
When specified limitations are exceeded, the ECU initiates an incident recording, which recovers the preceding 12 seconds and continues recording for 12 seconds afterward.
Weight and Balance
The helicopter had departed Stewart with 3 persons on board, plus 2 backpacks in the external basket on the right-hand side. The weight and balance were calculated by investigators using an estimated fuel load of 580 pounds, Footnote 5 which yielded a take-off weight of about 4300 pounds. The weight and centre of gravity were within prescribed limits.
Airworthiness
The helicopter had been in a previous accident on 15 December 2010, Footnote 6 and had sustained substantial damage. The helicopter had accumulated about 1290 hours of air time since new, and about 40 hours since returning to service following major repairs resulting from the previous accident. Maintenance records that were examined indicated that the helicopter was maintained in accordance with approved procedures. The daily inspection had been completed on the morning of the accident.
Wreckage Examination
Large sections of the cabin, the engine, the transmission and main-rotor hub with sections of main-rotor blades attached, the tail boom with sections of drive shaft, and the tail rotor and tail-rotor gearbox, were recovered. The tail-rotor driveshaft and the main driveshaft between the engine and transmission were severed. Separated sections of rotor blades were scattered across the face of the cliff. These sections of the rotor blades were not retrieved, due to the risks associated with their recovery. Passenger cameras, the handheld GPS, and the ELT were also recovered. In addition, the investigation was able to access the transmitted data from the GPS tracking system.
The helicopter was equipped with an ARTEX C406-N HM (part number 4543-5061, serial number 05613) ELT (installed and tested on 15 October 2010, function-checked on May 2011). The ELT was found to be active by recovery personnel 2 days after the occurrence, at which point it was turned off. The antenna was broken, and the antenna cable was severed. The Transportation Safety Board (TSB) has investigated numerous occurrences in the past 5 years where an ELT has been rendered ineffective due to damage to the unit or to the antenna. Footnote 7 In accordance with CARs Part V (Airworthiness) 551.104(f)(2)(ii), an ELT installed in a light helicopter must be mounted with its sensitive axis pointing approximately 45° downward from the normal forward direction of flight. However, in the accident aircraft, the ELT was mounted on a horizontal surface of the airframe, which formed the top of the pedestal between the 2 aft-facing passenger seats. The ELT model designator HM (Helicopter Model) is equipped with 6 gravity switches. The ELT was installed in accordance with the manufacturer's installation manual, which complies with CARs 551.104. No maintenance records were found regarding any repairs, modification, or replacement of the ELT antenna throughout the life of the helicopter.
The investigation was able to recover engine operating data from the occurrence helicopter's ECU. As a result, the engine was not disassembled for examination. The recorded data indicated that there were no FADEC faults recorded. ECU data, up to record 10 (Appendix A), indicated that the engine was operating normally, at torque values of between 58% and 62%, for at least 11 seconds before the torque declined to 52%. The decline was accompanied by a reduction of fuel flow and gas generator speed. Immediately thereafter, an incident recording was triggered by a loss of 9% main-rotor speed. The data showed that both the ECU and the pilot responded with control inputs that commanded the engine to accelerate at its maximum allowable rate. The engine did respond, and it reached its maximum fuel flow, during which time 5 consecutive torque exceedances were recorded. A subsequent sharp spike in torque reached 150%, and was followed by a divergence of power turbine and main-rotor speeds. Torque spikes are characteristic of rotor blades striking objects. Footnote 8
Performance calculations determined that the helicopter had more than enough power to hover out-of-ground effect at the existing weight, altitude, and temperature conditions, with engine anti-icing selected as off or on. Operation of engine anti-icing is required when outside air temperature is below 5°C in visible moisture. The temperature at the elevation of the exploration site was likely about 0°C. Video and still photography taken during the flight illustrate that the helicopter was not operating in or near visible moisture at the exploration site.
Examinations of recovered components and recordings, and research of systems, did not identify any pre-impact anomalies in the engine or drive-train components, the rotor blades, the flight-control components or the hydraulic system.
Flight Recorders
In March 2010, and again in June 2012, the TSB issued its Watchlist, which identified the safety issues investigated by the TSB that pose the greatest risk to Canadians. A multi-modal problem identified in the Watchlist is that “data critical to understanding how and why transportation accidents happen are frequently lost, damaged, or not required to be collected.” Single-engine turbine-powered helicopters requiring only 1 pilot, such as the Bell 407, do not meet the cockpit voice recorder (CVR) and flight data recorder (FDR) provisions of CARs 605.33, and are not required to have these recorders installed. The occurrence helicopter was not equipped with either a CVR or a FDR. As a result, information from these devices was not available to TSB investigators.
The last 2 minutes of recorded handheld GPS data showed that the helicopter came to a stationary position and altitude for 54 seconds before electrical power was interrupted or the GPS signal was lost. The next position report would have been recorded 6 seconds later.
Information gathered from the digital video and still cameras, the handheld GPS, and the GPS tracking system were invaluable to the TSB investigation. There have been significant technological advances in the past several years; a large number of miniature data, video, and audio-recording devices are available to the general public. These miniature recording devices overcome many of the limitations of older generation recorders in terms of size, weight, and storage capacity. It is now possible to have full high-definition video recorders that are smaller than a traditional point-and-shoot 35-mm camera.
Fuel
Daily fuel samples from the helicopter fuel filter, the dispensing fuel filter, and the storage tank from the day of the accident were clear and clean to the naked eye, and a test dye-stick did not detect evidence of water or de-icing fluid in the samples. The accident flight was the first flight of the day. The flight operated for about 21 minutes before the accident. Other helicopters using the same fuel source that day did not experience any fuel-related problems.
Flight- and Duty-time Limitations
The operator's directives on flight- and duty-time limitations reflect those found in the CARs. COM 4.25.1.1 describes standard flight-time limitations, including a maximum of 120 hours in any 30 consecutive days, and 60 hours in any 7 consecutive days.
COM 4.25.1.2 states that pilots shall not work more than 14 hours in any consecutive 24 hours. In addition, COM 4.25.1.4 states that each pilot shall have at least 1 period of 24 hours free from duty 3 times within each 30 consecutive days, and 13 times within each 90 consecutive days.
Aircrew
The pilot held a commercial pilot licence (helicopter), originally issued in 2001. The licence was restricted to daylight flying, and was validated by a Category 1 aviation medical examination. The licence was valid to 01 July 2012, with no medical limitations. The investigation determined that there was nothing to indicate that the pilot's performance was degraded by pre-existing medical conditions.
The pilot was hired by VIH Helicopters Ltd. in January 2011. At the time of the accident, records indicated that the pilot had accumulated approximately 2500 flight hours as PIC in various light single-engine helicopters, and another 1000 flight hours as PIC in multi-engine helicopters. The pilot's training records indicate that VIH Helicopters Ltd. provided the pilot with type training and an endorsement on the Bell 407 helicopter, plus hover-exit training, in January 2011. A familiarization flight in the area north of Stewart was completed with the operator chief pilot in June 2011. A previous employer provided crew resource management (CRM) and pilot decision-making training in 2010, and mountain flying training in 2008. The occurrence pilot had accumulated approximately 240 flight hours of mountain flying work, involving crew changes, toe-in operations and external loads in support of mineral exploration projects.
With the exception of one 15.1-hour duty day on 17 July 2011, recorded flight- and duty-times did not exceed limitations during the pilot's tour (see Crew Scheduling). In the 15 days preceding the accident, the average length of the pilot's duty day was 12.75 hours. Duty days on 28 and 29 July were 12.75 hours each, with 5.6 hours of flight time each day. On 30 July, the pilot was on duty for 11.5 hours, flying 6 flights and logging 3.8 hours of flight time. These recorded duty-day times cover the daily period between first departure and last landing, and do not include allowance for pre-flight or post-flight duties. The VIH Helicopters Ltd. COM (in accordance with CARs 700.16 [1]) limits a pilot's workday to 14 hours in any 24-hour period. The operator provides forms that record the entire duty day. The pilot had not yet completed the form, which was to be submitted monthly. Every day included several periods of more than 30 minutes between flights. On 1 occasion, there was a break of 4.5 hours between flights. These break periods, as well as departure times, were completely random. During the occurrence pilot's tour, approximately 100 flight hours were accumulated, reaching a maximum of 40 hours over any 7-day period.
The occurrence pilot stayed at base camps during the tour. The camps were described as comfortable, with good bedding and good food. The pilot stayed at an operator staff house in Stewart on the night before the accident. On the morning of the accident, the pilot appeared to be rested and in good spirits.
Crew Scheduling
The normal rotation for this project was a 4-week tour followed by 2 weeks of leave. In some cases, tour lengths were extended to meet operational requirements or to accommodate leave requests of other pilots. The occurrence pilot commenced a 3-week tour on 12 July 2011, after an extended leave of 27 days off. The pilot had requested the extended period of leave, which was approved by the employer. The 3-week tour was part of an operator effort to realign pilots' schedules back to the 4-on/2-off rotation. On 28 July 2011, the occurrence pilot was advised that the tour would have to be extended by 10 days. The pilot was to Stewart on 30 July to accommodate a leave request made by another pilot. In response to this request, the pilot expressed deep frustration with the extension and the short notice of it.
The area surrounding Stewart is an active area for mineral exploration. The terrain is very rugged, and pilots perform operations such as toe-in landings and hover exits/entries, as well as external-load operations in support of mineral-exploration activities. Many flying days are lost because of weather. The investigation determined that the occurrence pilot felt that the work in Stewart was very demanding, and that pilot fatigue could make it unsafe near the end of a 4-week tour. The pilot had also expressed displeasure about the fact that the tour had been extended just before the pilot was scheduled to leave, and felt that such an extension affected a person's ability to focus on the job and also caused problems at home. On at least 1 previous occasion, the pilot had requested to be relieved due to fatigue. In that instance, the VIH Helicopters Ltd. scheduler arranged for a relief pilot to arrive within 2 days. The investigation determined that the operator supported a pilot's decision not to fly due to concerns about being tired, and it was not an issue for the exploration group to postpone work to allow a pilot to get some additional rest. The occurrence pilot did not request that work be postponed, nor indicate a need to be relieved from the current tour due to fatigue.
The pilot arrived in Stewart on the day before the accident, which was the pilot's nineteenth day of work. The pilot was new to the Nelson Glacier project. A crew-change briefing was provided by the outgoing pilot; it covered the location and description of the work sites, and provided a map review of low weather routes. The occurrence pilot declined an offer of a familiarization flight. At the end of that day, the occurrence pilot picked up 4 passengers at other sites, plus the 2-person exploration crew from the Nelson Glacier site, and returned them to Stewart. The occurrence flight was the pilot's second trip to that site.
Survivability
Both seats in the pilot compartment were equipped with a 4-point restraint system. The pilot remained restrained, by the lap belt and shoulder straps, in the seat throughout the accident sequence. The pilot was wearing a helmet.
The passenger in the left front seat was found free of the helicopter. The restraint system was attached to the airframe independently of the seat, and was found with the lap belt and both shoulder belts buckled up. The seat remained in the helicopter. The outboard end of the lap belt was secured to its attachment point on the aft door post. The door post had separated at its base from the airframe as the airframe came apart, creating an opening in the side of the helicopter next to the then-unrestrained passenger.
The rear-seat passenger was also found free of the helicopter. All seat restraints in the passenger compartment were equipped with 3-point restraint systems, and all were found unfastened.
The forces associated with the break-up following impact with the terrain were severe and beyond the extremes of normal human tolerance. The collision with the terrain was not survivable.
Operator
VIH Helicopters Ltd. is a subsidiary of VIH Aviation Group. VIH Helicopters Ltd. operates a fleet of 40 helicopters in domestic and international operations, and provides the majority of its services under aerial work (CARs Part VII, Subpart 2) or air taxi operations (CARs Part VII, Subpart 3). VIH Helicopters Ltd. has initiated work toward implementing a formal safety management system (SMS); however, the company is not currently required by regulation to have a fully implemented SMS.
In its safety policy, VIH Helicopters Ltd. considers safety to be a core value, and imposes upon its employees not only a right but a responsibility to refuse work when unsafe conditions or risk of imminent harm exist. The investigation determined that VIH Helicopters Ltd. had previously supported employees who identified unsafe working conditions and had taken the necessary steps to mitigate risk to acceptable levels.
SMS is another area identified in the TSB Watchlist. As stated in the TSB Watchlist,
Implemented properly, safety management systems (SMS) allow transportation companies to identify hazards, manage risks, and develop and follow effective safety processes. However, Transport Canada does not always provide effective oversight of transportation companies transitioning to SMS, while some companies are not even required to have one.
The following TSB laboratory reports were completed:
- LP098/2011 – Engine instrument analysis
- LP099/2011 – Sequential time sequence
- LP104/2011 – Audio enhancement
These reports are available from the TSB upon request.
Analysis
There were no witnesses to the occurrence, and there were no cockpit voice recorder (CVR) or flight data recorder (FDR) data to assist investigators. Information gathered from the electronic control unit (ECU), the global positioning system (GPS) tracking system, the portable GPS, and the personal cameras greatly assisted the TSB investigation. There is no indication that a helicopter system failure or malfunction contributed to this occurrence. As a result, this analysis focuses on a possible scenario for why the helicopter struck terrain. In addition, the analysis will also discuss several factors related to flight-following procedures and overdue-aircraft response plans, in an effort to enhance safety.
The recorded GPS data showed the helicopter in, or near, a stationary hover for 54 seconds until electrical power was interrupted, or the GPS signal was lost. The ECU data indicated a small, gradual power reduction, followed by a sudden reduction in main-rotor rpm. It is likely that the decrease in main-rotor speed occurred as a result of the main-rotor blades making contact with an obstacle as the helicopter manoeuvred in close proximity to the rock face. Any damage to rotor blades, which provide both a supporting and a control surface, is likely to result in an unstable control condition or a complete loss of control. The sudden increase in torque to 150% is consistent with a significant rotor strike. The subsequent divergence of the main-rotor speed (decreased) and power turbine speed (increased) is indicative of a sudden release of torque due to severing of the driveshaft between the engine and the transmission. While working in close proximity to steep terrain, for undetermined reasons, the helicopter's main-rotor blades made contact with terrain, causing a subsequent loss of control and collision with terrain.
Flight following is a defence against potential adverse consequences when an aircraft goes missing or is overdue. This defence began to break down when the verbal flight plan did not provide a specific time of return to Stewart. In the absence of a documented operational flight plan, a means of recording changes to that flight plan, and explicit guidance on when a flight is to be considered overdue, assumptions made by ground personnel about the status of an aircraft may lead to delays in initiating the overdue-aircraft response plan. Although communications were attempted, it was known that communication coverage was intermittent. When there is a gap between operator procedures and actual practice, flight crew and passengers may be placed at increased risk for injury or death following an accident.
An emergency locator transmitter (ELT) is another defence that can aid in reducing delays in the initiation of search and rescue. This defence failed when the antenna was broken and the antenna cable was severed. As a result, the ELT signal was not detected by the Canadian Mission Control Centre. The operator's ground personnel believed that they would have been contacted by the Joint Rescue Coordination Centre (JRCC) if the occurrence helicopter had been in an accident. Damage to the ELT or its antenna increases the likelihood that a distress signal will not be detected. As a result, injured flight crew and passengers will be at elevated risk for death due to delays in life-saving search-and-rescue services. Operator procedures and personnel involved in flight following need to take account of the limitations of ELTs.
The occurrence aircraft was equipped with a GPS tracking system, which provided position updates every 2 minutes. The system did not include any means of automatic emergency notification. In this occurrence, ground personnel did not receive a manually activated emergency notification via the GPS tracking system, which contributed to the belief that the occurrence pilot had landed to wait for the weather to improve. According to the company operations manual (COM), the overdue-aircraft response plan should have been initiated when the aircraft was considered to be overdue. However, the absence of a reported ELT signal, combined with having not received an emergency notification via the GPS tracking system, led ground personnel to believe that the situation did not warrant initiating the overdue-aircraft response plan. This belief contributed to the delay in initiation of search-and-rescue action. The operator's overdue-aircraft response plan required that the JRCC be notified that search-and-rescue services may be required. This step did not occur, and the JRCC was not notified of the overdue aircraft. If the JRCC is not notified in a timely manner, the flight crew and passengers of that aircraft are placed at increased risk for injury or death as a result of delays in potentially critical life-saving search-and-rescue services.
Consecutive days of work can have a cumulative effect on fatigue in helicopter pilots, particularly when the work involves tasks that require high levels of concentration, increasing the pilot's workload. Footnote 9 Cumulative fatigue can build up when a sleep debt is carried over from preceding days of inadequate sleep. Footnote 10
The occurrence pilot had indicated concerns about 4-week tour lengths, due to the demanding nature of the job. The investigation determined that there may have been a conflict between the pilot's personal plans and the employer's operational needs. This conflict may have been the catalyst for the pilot to express frustration to operator personnel and relate it to flight-safety concerns. However, there was no indication that the pilot was experiencing the effects of fatigue at the time of the occurrence. In the days before the occurrence, the pilot's flying times and duty days were within the prescribed limits as per regulations. On the morning of the occurrence, the pilot was in good spirits and appeared well rested. In addition, the pilot had not indicated to the operator or the exploration group, as he had done on a previous tour, that he was experiencing the effects of fatigue. The investigation did not establish a link between 4-week tour lengths and pilot fatigue in this occurrence.
The occupant restraints of the rear cabin seats were not fastened. It is possible that the passenger in the rear seat had unfastened that seat's restraint in anticipation of carrying out a hover exit near the accident site, and that the restraint was not used again when the passenger re-entered the helicopter after retrieving the climbing rope. Or it is possible that the restraint was not used at all for the duration of the flight. During flight operations, restraint systems should be used, and should be released only when required for the occupant to exit the aircraft. Procedures such as toe-in landings and hover exits require passengers to release their restraint systems. Passengers conducting hover exits are at increased risk for injury if restraint systems are unfastened for periods longer than necessary.
The helicopter was equipped with a GPS tracking system with a reporting frequency of 2 minutes. More frequent reporting may have provided additional data useful for the investigation. In addition to the GPS tracking system, 3 other sources of recorded data provided additional information of immense value to the investigation: a portable GPS, handheld digital cameras, and the aircraft's ECU.
Many types of miniature data, video and audio-recording devices have become available in recent years. The helicopter was not required by regulation to be equipped with any type of flight-information recording devices. This lack of requirement may limit the amount and quality of data that can be gathered during an investigation.
Findings
Findings as to causes and contributing factors
- While working in close proximity to steep terrain, the helicopter's main-rotor blades made contact with terrain, causing a subsequent loss of control and collision with terrain.
- When there is a gap between operator procedures and actual practice, flight crew and passengers may be placed at increased risk of injury or death following an accident.
- If the Joint Rescue Coordination Centre is not notified in a timely manner once an aircraft is determined to be overdue or has been involved in an accident, the flight crew and passengers of that aircraft are placed at increased risk for injury or death as a result of delays in potentially critical, life-saving search-and-rescue services.
- Damage to the emergency locator transmitter or its antenna increases the likelihood that a distress signal will not be detected. As a result, injured flight crew and passengers will be at elevated risk for death due to delays in life-saving search-and-rescue services.
- Procedures such as toe-in landings and hover exits require passengers to release their restraint systems. Passengers conducting hover exits are at increased risk for injury if restraint systems are unfastened for periods longer than necessary.
- If cockpit or data recordings are not available to an investigation, this may preclude the identification and communication of safety deficiencies to advance transportation safety.
Other findings
- The investigation did not establish a link between 4-week tour lengths and pilot fatigue in this occurrence.
Safety action
Safety action taken
VIH Helicopters Ltd. has undertaken efforts to work with manufacturers of flight data monitoring systems to develop and test vendor hardware and software that would further meet the needs of VFR helicopter operations.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A - ECU Recorded Data

Definitions for chart
- PLA
- Throttle
- MGT
- Measured gas temperature
- Np/Nr
- Power turbine speed / Main-rotor speed
- Ng
- Gas generator speed
- Q
- Torque
- Cp
- Collective pitch
- Fuel flow
- Engine fuel flow
- Pph
- Pounds per hour