Loss of control on landing
Sudbury Aviation Limited
de Havilland DHC-2 Mk. I, C-FHVT
Kennedy Lake, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Sudbury Aviation Limited float-equipped de Havilland DHC-2 Beaver aircraft (registration C-FHVT, serial number 284) was on approach to Kennedy Lake, Ontario, with the pilot and 2 passengers on board, when the aircraft rolled to the left prior to the flare. The pilot attempted to regain control of the aircraft by applying full right rudder and right aileron. The attempt was unsuccessful and the aircraft struck rising tree-covered terrain above the shoreline. The aircraft came to a stop on its right side and on a slope. The pilot and the passenger in the rear seat received minor injuries. The passenger in the right front seat was not injured. All were able to walk to the company fishing camp on the lake. There was no fire and the 406 megahertz emergency locator transmitter (ELT) was manually activated by one of the passengers. One of the operator's other aircraft, a Cessna 185, flew to the lake after C-FHVT became overdue. A search and rescue aircraft, responding to the ELT, also located the accident site. Radio contact between the Cessna 185 and the search and rescue aircraft confirmed that their assistance would not be required. The accident occurred at 1425 Eastern Daylight Time.
Le présent rapport est également disponible en français.
Factual information
History of the flight
Sudbury Aviation Limited operates several fishing camps located at different lakes in Northern Ontario. Twice a week, 1 of the company's 2 de Havilland Beaver aircraft flies to the camps to check on the guests and provide supplies they require, or to set up camps with supplies for incoming guests. On the occurrence flight on 25 June 2014, the float-equipped de Havilland DHC-2 Beaver aircraft (registration C-FHVT, serial number 284) was to visit 3 camps; the aircraft was loaded with refreshments, additional fuel for outboard motors, and 2 outboard motors that were destined for the Kennedy Lake camp.
In addition to the pilot, the company’s chief pilot was sitting in the right front seat as a passenger, and a dockhand was sitting in the middle of the rear bench seat. All 3 occupants were wearing lap belts. Shoulder harnesses were available for the 2 front seats, but were not worn.
The flights to the first 2 camps were uneventful. En route to Kennedy Lake, the aircraft approached the camp from the northeast and circled overhead the camp while descending, which allowed the pilot to assess the wind and water conditions.
Kennedy Lake is long and narrow, with rising terrain from either side of the shoreline. Most of the shoreline is tree-covered, with some sections having vertical rock faces.
Landing flaps were selected as the aircraft descended below the tree tops. As it entered the narrow section of the lake, the aircraft yawed to the left, and the left wing dropped just prior to the flare. The pilot tried to counteract with right rudder and right aileron, but was not successful. The aircraft continued its heading to the rising shoreline and struck the terrain and trees in a slight nose-up attitude with the wings level. The accident occurred at 1425 Eastern Daylight Time.
After coming to a stop, the aircraft was leaning to the right such that the right front and cabin doors faced down the slope (Photo 1). The right wing had separated from the fuselage. There was concern that the aircraft could slide down the slope and caution was taken while moving inside the cabin towards the left cabin door. The 3 occupants exited the aircraft through the left cabin door, which they were able to open only partially, as the substantially damaged left wing was blocking it.

Before exiting, the chief pilot attempted to transmit on the radio using the 121.5 megahertz frequency, but received no response. The pilot and chief pilot secured the aircraft before exiting, and the chief pilot selected the emergency locator transmitter (ELT) to the “ON” position.
The survival pack, first aid kit, and water bottles were retrieved from the aircraft before the 3 occupants began walking to the nearby camp. A company Cessna 185 arrived some time later and began transporting the occupants back to their base. Search and rescue (SAR) aircraft, responding to the ELT, contacted the Cessna 185. Once it was determined their services were not required, the SAR aircraft departed the scene.
Pilot information
Records indicate that the pilot was certified and qualified for the flight in accordance with existing regulations. The pilot had held a commercial licence since 1990. The pilot held a valid medical certificate with the only restriction that glasses must be worn. The pilot’s flying experience was estimated to be 3500 hours, with approximately 1000 hours on C-FHVT. The total flying time per year was approximately 140 hours as pilot-in-command of C-FHVT.
Sudbury Aviation Limited
Sudbury Aviation Limited operates 2 DHC-2 Beaver aircraft, a Cessna 172, and a Cessna 185 in accordance with Canadian Aviation Regulations (CARs) Subpart 703. It transports passengers and supplies from the Sudbury base to various fishing camps from May to early November. Sudbury Aviation Limited is currently not required by regulation to operate with a safety management system (SMS).
Weather
Visual meteorological conditions (VMC) existed at the time of the accident. The 1400 aviation routine weather report (METAR) for Sudbury, Ontario, which is approximately 40 nautical miles south of Kennedy Lake, was temperature 20 °C, dew point 8 °C, wind 020° true (T) at 12 knots, gusting to 19 knots under a mostly cloudy sky. There was no precipitation, and visibility was unlimited. There was no weather reporting station near Kennedy Lake. The pilot reported the wind as variable and gusting from the west. Topography surrounding the lake can affect wind direction and velocity almost instantly on the windward side of the lake. The magnetic variation at Kennedy Lake is 12 degrees west.
Kennedy Lake and aircraft location
Kennedy Lake has a narrow middle section and wider open water areas at both ends of the lake. The lake is oriented on a 300/120º magnetic heading, with rising tree-covered terrain on either side of the shoreline. At the accident location (Figure 1), the height of the slope above the lake surface was approximately 50 feet, with trees of approximately 30 feet in height. The aircraft came to rest approximately 30 feet above the water surface. The width of the lake at the landing site was estimated to be 170 feet. The aircraft's wingspan is 48 feet, which leaves approximately 60 feet between the wingtip and the shoreline on either side of the aircraft. The topography surrounding Kennedy Lake directly affects wind conditions and causes wind direction to shift rapidly, especially in gusty conditions. This becomes more noticeable when an aircraft descends below the tree line or is on the lake surface.

Aircraft information
The aircraft was certified, maintained, and equipped in accordance with existing regulations, and was being operated within the weight and balance limitations set out in the pilot operating handbook.
The majority of the maintenance and inspections were performed prior to the aircraft entering service in the spring of each year. There were no pre-impact airframe failures or system malfunctions. Propeller blade damage and twist were consistent with power being produced at the time of impact.
The airspeed indicator (ASI) was removed and shipped to the TSB laboratory to determine airspeed at impact. The examination revealed that the impact forces during the accident sequence had been insufficient to deform the ASI pointer or generate any physical signature on the faceplate of the instrument that would make it possible to determine the airspeed at the time of impact.
The restraint system was examined after information was received that the company pilots were not wearing shoulder harnesses on most flights. The shoulder harness on this aircraft is a separate strap that pulls down from a roof-mounted inertia reel and latches onto the lap-belt buckle; it is available to the front-seat occupants only. The reason given for the shoulder harness not being worn was that when it was latched to the lap belt, pilots were unable to reach the water rudder lever—even when the inertial reel was at full extension. To reach the water rudder lever, pilots have to unlatch the shoulder harness before starting the take-off run, and again after landing before taxiing. Another complication is that the fully retracted shoulder harness is awkward to reach from the pilot seat.
The shoulder harness was installed in 1995 in accordance with Supplemental Type Certificate (STC) SA711GL and Advisory Circular (AC) 43-13-1A.
The shoulder harness installation on the operator’s second Beaver aircraft was examined because it was an identical installation. A pilot of average height was seated in the left front seat. It was clear that with the shoulder harness latched and at full extension, the water rudders were difficult to reach. Measurements were taken of the shoulder harness and the buckle end of the lap belt at full extension. The measurements were compared to the measurements provided by the STC holder, Wipaire, Incorporated. The shoulder harness part number was the part number listed on the STC. At full extension, the shoulder harness measured 59 inches. An STC note for the shoulder harness specification reads, “to be 1500 lb. rated, 66” long-min, fixed or inertia reel”.
Canadian Aviation Regulations 605.25(1) states that the pilot-in-command shall direct all persons on board the aircraft to fasten safety belts during movement of the aircraft on the surface, during take-off and landing, and any time during the flight that the pilot-in-command considers it necessary that safety belts be fastened. CARs 605.27(1) states that crew members seated at their stations shall have available safety belts fastened. In addition, Transport Canada (TC) published Civil Aviation Safety Alert 2013-09 to clarify the requirements of these regulations. In November 2014, TC issued Advisory Circular (AC) 605-004, titled “Use of Safety Belts and Shoulder Harnesses on Board Aircraft”. Section 3 of the AC provides information on the use shoulder harnesses on small aircraft, requirements for the installation of shoulder harnesses, and their proper use. The statistical information for the AC was derived from TSB accident reports that had identified how shoulder harnesses might have prevented serious injuries during an accident.
During the investigation into the 25 May 2012 de Havilland DHC2 accident at Lillabelle Lake, Ontario (TSB Aviation Investigation Report A12O0071), the TSB reviewed accident and injury data from a number of float plane accidents. The TSB considered that, given the additional hazards associated with accidents on water, shoulder harnesses for all seaplane passengers would reduce the risk of incapacitating injury, thereby improving their ability to exit the aircraft. Therefore, the Board recommended that
The Department of Transport require that all seaplanes in commercial service certificated for 9 or fewer passengers be fitted with seatbelts that include shoulder harnesses on all passenger seats.
Transportation Safety Recommendation A13-03
In its response to the recommendation, Footnote 1 TC indicated that the cabin designs and configurations of most of the commercially operated float planes in Canada likely do not readily lend themselves to installation of shoulder restraints for all passengers without substantial aeroplane redesign and/or structural modification.
As the TSB observed in its assessment of TC’s response, there are approximately 600 aircraft on the Canadian commercial aircraft registry that are potentially operated on floats, certificated for 9 or fewer passengers and manufactured before 1986. Of these aircraft, approximately 200 are DHC-2s and 300 are Cessnas. There are already shoulder harness installation kits available for the Cessna’s as described in Cessna Single Engine Service Bulletin SEB92-28. Additionally, TC approved a Limited Supplementary Type Certificate (O-LSA09-360/D) for the installation of rear shoulder harnesses in several DHC-2’s in 2009. These facts support the feasibility of retrofitting many floatplane designs with shoulder harnesses.
In its response to Recommendation A13-03, TC also stated that most of the aircraft structures are not robust enough to support shoulder restraints in a crash and may hinder egress. The TSB remarked, however, that TC had not demonstrated that the risk of hindering egress outweighed the benefits of rear-seat shoulder harnesses. It observed that shoulder harnesses in all seating positions for normal/utility category of aircraft had been required by regulation since 1986, and had been installed since that time in similar—albeit newer—aircraft to the ones previously described. The TSB inferred from the availability of these installations, the existing kits, and TC-issued Supplemental Type Certificates (STC’s) that the aircraft structures are robust enough to support these restraints.
Transport Canada, the TSB has concluded, has not given details of any action taken or proposed that would reduce or eliminate the safety deficiency; provided any objective information to demonstrate that it is not feasible to install rear-seat shoulder harnesses; or demonstrated that the risk would not be reduced significantly if rear-seat shoulder harnesses were installed. Consequently, the Board believes that the risks identified in Recommendation A13-03 have not abated and remain significant, and considers TC’s response to Recommendation A13-03 to remain Unsatisfactory.
Stall characteristics
As aircraft are on approach to land, power is reduced, and the angle of attack is increased to reduce airspeed. To meet performance specifications, the DHC-2 Beaver flight manual suggests a final approach speed of 1.3 times the stall speed. Footnote 2
An aircraft wing stalls at a specific angle of attack. Rapid changes in wind speed or direction or mechanical turbulence caused by geographic features can cause disruptions to the normal airflow over the wing. These disruptions can result in portions of the wing exceeding the stalling angle of attack.
The flight manual indicates a stall speed with landing flaps of 45 mph indicated airspeed, and that, during the stall, "If yaw is permitted, the aircraft has a tendency to roll. Prompt corrective action must be initiated to prevent the roll from developing." Footnote 3
When C-FHVT was originally certified there was no requirement to include a stall warning system, and none was originally installed on the aircraft. A stall warning system is a device that provides a clear and distinguishable stall warning to the pilot, which is independent of the pilot’s recognition of inherent aerodynamic qualities near the stall, such as buffeting. Viking Air Limited (VAL), the current holder of the DHC-2 type certificate, has designed a modification (STC# SA92-63) which includes the installation of a stall warning system on the DHC-2 aircraft. However the installation is not mandated and was not installed.
The TSB has previously identified stalls encountered during critical phases of flight as having potentially disastrous consequences, and is concerned that the aerodynamic buffet of DHC-2 aircraft alone may provide insufficient warning to pilots of an impending stall.
Transport Canada has published Civil Aviation Safety Alert (CASA) 2014-02 that advises owners, operators and maintainers of the availability, and recommends the installation, of an artificial stall warning system for DHC-2 series aircraft.
Bench seat and floor attachments
The bench seat and its floor attachments were examined. The bench seat appears to be part of an STC incorporated on the aircraft at some time during its service life. The left-rear of the seat had been attached by 2 anchors through the floor to the floor-support beam. A section of floor containing the anchors as well as part of the floor-support beam were found detached (Photo 2 and Photo 3).
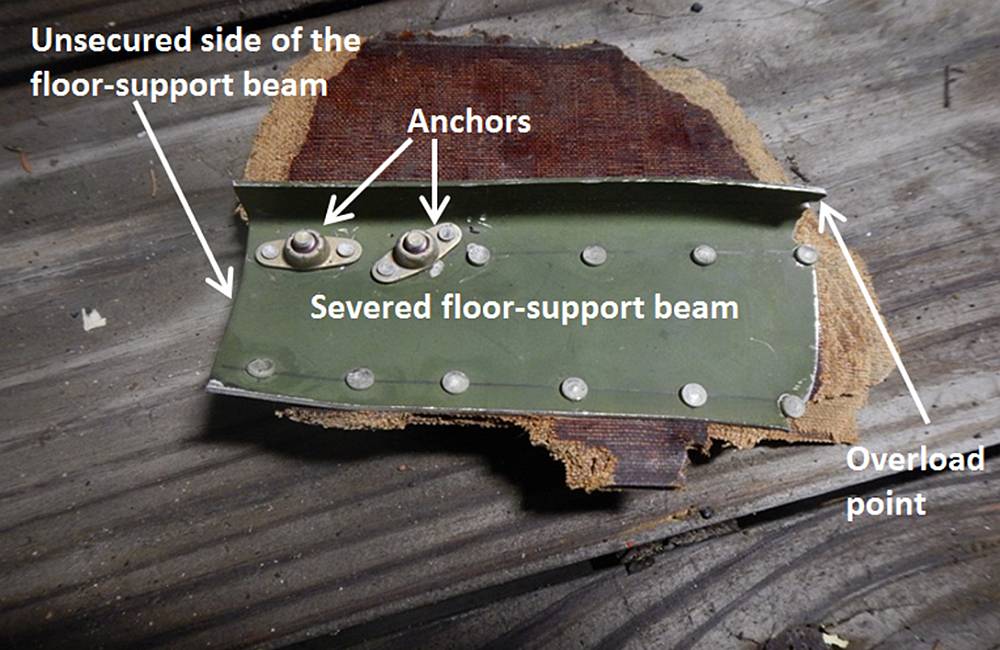
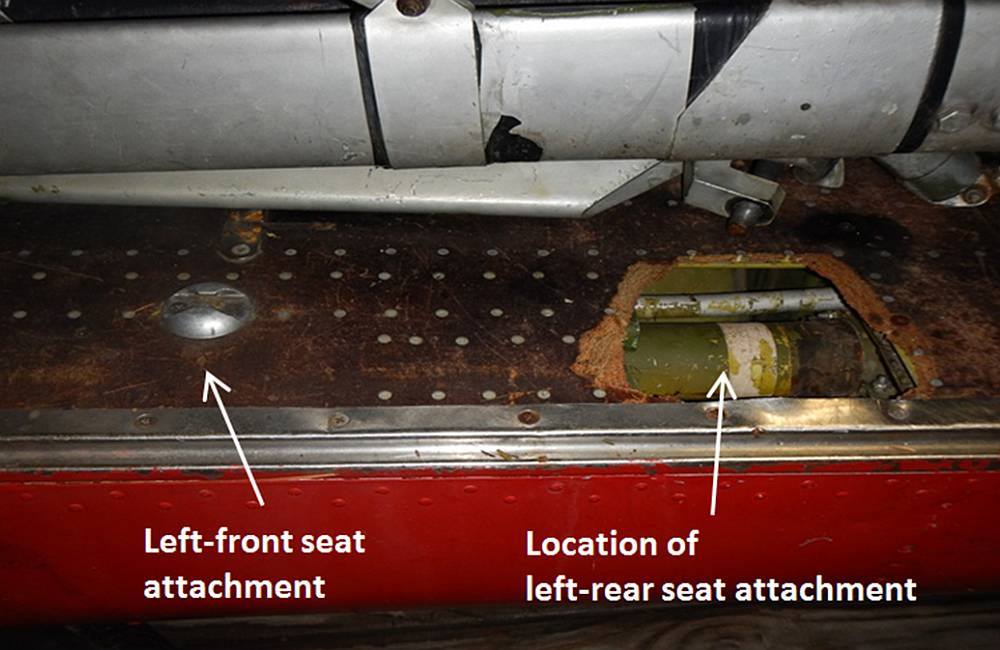
Further examination determined that the rear of the floor-support beam had not been secured or supported, which allowed the seat and its attachment to bend and fail in overload in a forward direction during the impact.
In August 1984, de Havilland Aircraft Company issued Service Bulletin 2/39 for DHC-2 Mk.I, Mk.II, and Mk.III Turbo Beaver aircraft. The Service Bulletin was issued following accident and incident reports indicating "the use of unapproved seats with inadequate strength, improper repairs on approved seats, unserviceable or improperly installed floor attachments, (…) [and] inadequate strength seat belt attachments" installed on their aircraft. The Service Bulletin recommends that during every 100-hour inspection, the seat, seat belts, floor attachments and reinforcements be checked for integrity, especially when those seats are frequently removed to provide additional space for carrying freight.
TSB laboratory reports
The following TSB laboratory report was completed in support of this investigation:
- LP134/2014 – Airspeed Indicator Examination
Analysis
The pilot was qualified for the flight and no mechanical discrepancies that would have affected control of the aircraft were reported or found during the examination. This analysis will focus on the particular circumstances that led to the aircraft impacting the terrain and safety related factors that can affect the safety of the flight and passengers during an accident.
As the aircraft approached the lake for landing and landing flap was lowered, airspeed was reduced towards the final approach speed.
The wind surrounding the landing surface was gusty and was significantly affected by the geographic features, which cause rapid changes in wind speed and direction, and mechanical turbulence.
When the aircraft was relatively close to the surface it encountered a westerly gust. This caused the aircraft to yaw to the left which decreased airflow over the left wing surface and effectively increased the angle of attack.
The left wing entered an aerodynamic stall and dropped. There was little time for corrective action by the pilot due to the proximity of the rising shoreline on either side. The attempt to counter the un-commanded left roll and initiate a climb was unsuccessful and the aircraft struck the trees.
If an aircraft is not equipped with a stall warning system, there is an increased risk that the pilot may not be aware of an impending aerodynamic stall.
The investigation determined that company pilots were not wearing their shoulder harnesses since the harness restricted their ability to operate the water rudders. A review of Supplemental Type Certificate (STC) SA711GL for the shoulder harness installation determined that the shoulder harness assembly was the correct part number. However, the shoulder harness was short when fully extended and would not allow for the 66-inch minimum extension clearance noted in the STC. If a shoulder harness is installed that restricts pilot movement, and, as a result, their ability to reach the water rudders, there is a risk that the pilot will not use it. If a shoulder harness is not worn, there is an increased risk of injury or death in an accident.
The bench seat aft floor mount attachment was secured to the underfloor beam, but the beam was not secured on the aft side and failed in bending overload during the impact. Although the lap belt was worn, it was attached to the seat and did not prevent the occupant from shifting forward with the seat. This resulted in minor injury to the passenger in the rear seat.
Findings
Findings as to causes and contributing factors
- Prior to touchdown in a northerly direction, the aircraft encountered a gusty westerly crosswind and the associated turbulence. This initiated an un-commanded yaw and left wing drop indicating an aerodynamic stall. The pilot was unsuccessful in recovering full control of the aircraft and it impacted rising terrain on the shore approximately 30 feet above the water surface.
- The rear bench seat floor support attachment failed in overload and did not prevent the seat or its occupant from moving forward during the impact, which resulted in minor injury to the passenger in the rear seat.
Findings as to risk
- If a shoulder harness is installed that restricts pilot movement, and, as a result, their ability to reach the water rudders, there is a risk that the pilot will not use it.
- If a shoulder harness is not worn, there is an increased risk of injury or death in an accident.
- If an aircraft is not equipped with a stall warning system, there is an increased risk that the pilot may not be aware of an impending aerodynamic stall.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .