Loss of control and collision with terrain
MAG Aerospace Canada Corp.
Rockwell International Aero Commander 690B, C-GYLD
Thunder Bay Airport, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
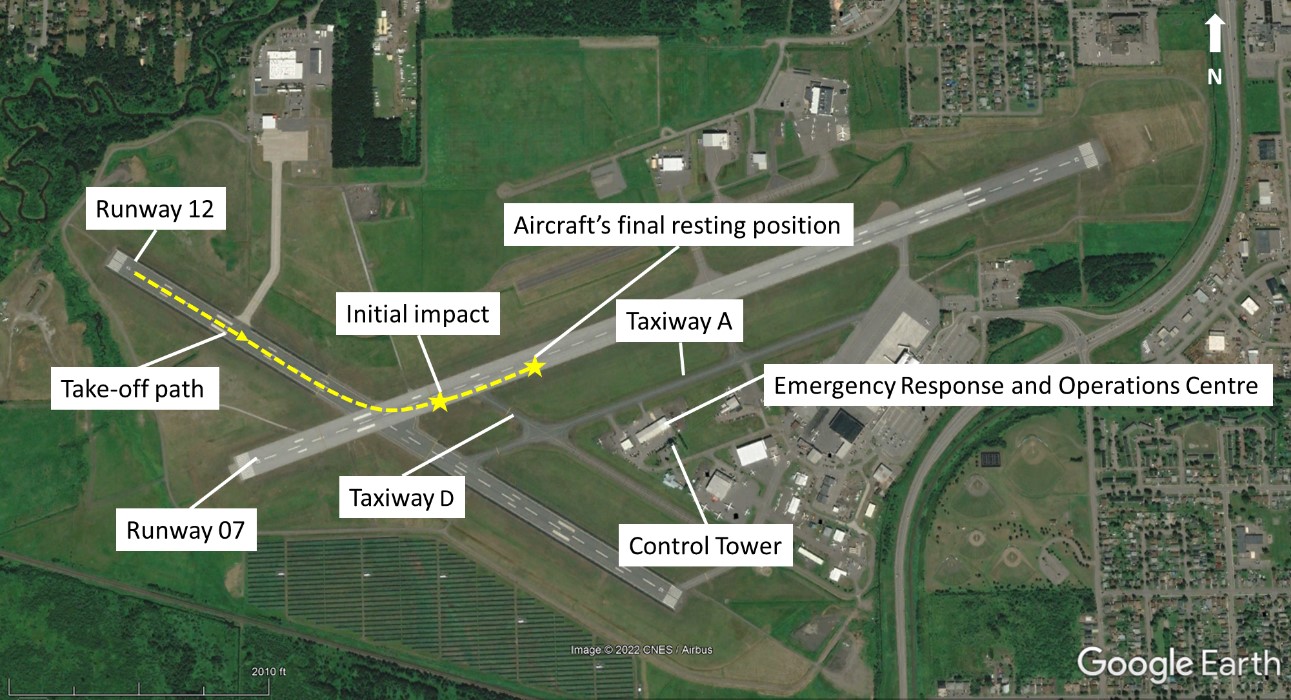
On 16 August 2021, the Rockwell International Aero Commander 690B aircraft (registration C-GYLD, serial number 11426), operated by MAG Aerospace Canada Corp. as flight BD160, was conducting a visual flight rules flight from Thunder Bay Airport, Ontario, to Dryden Regional Airport, Ontario, with only the pilot on board. At 2109 Eastern Daylight Time, the aircraft began a takeoff on Runway 12. Shortly after rotation, the aircraft entered a left bank, continued to roll, and then struck the surface of Runway 07 in an inverted attitude. The pilot was fatally injured. The aircraft was destroyed by the impact and post-impact fire. The emergency locator transmitter activated on impact.
1.0 Factual information
1.1 History of the flight
1.1.1 Occurrence flight
On 16 August 2021, the MAG Aerospace Canada Corp. (MAG Canada) Rockwell International Aero Commander 690B aircraft (registration C-GYLD, serial number 11426) was conducting bird dog flightFootnote 1 160 (BD160), in accordance with visual flight rules (VFR), between Thunder Bay Airport (CYQT), Ontario, and Dryden Regional Airport (CYHD), Ontario, with only the pilot on board. This was the pilot’s 3rd flight of the day. The aircraft had been refuelled at CYQT and was to be flown to the operator’s facility at CYHD for maintenance.
The occurrence pilot taxied the aircraft to Runway 12 and then held short. At 2106:17,Footnote 2 CYQT air traffic control (ATC) instructed the pilot to line up on Runway 12.
At 2106:31, ATC cleared an incoming aircraft for landing on Runway 25. Before that aircraft landed, the occurrence pilot and the pilot of the incoming aircraft had a brief and informal discussion over the ATC frequency. After the incoming aircraft landed at 2108:47, ATC instructed it to exit the runway onto Taxiway D.
At 2109:17, the occurrence pilot was cleared for takeoff with the option of either a left or right turnout. The aircraft began its takeoff at 2109:22 and, immediately after rotation, it entered a climbing left turn. When it was approximately 45 feet above ground level (AGL), the aircraft entered a rapid roll to the left.
At 2109:50, the aircraft struck the surface of Runway 07 in an inverted attitude (Figure 1). The pilot was fatally injured. The aircraft was destroyed by the impact and post-impact fire. The emergency locator transmitter activated on impact.
The occurrence flight was captured by a video camera mounted on the Emergency Response and Operations Centre at CYQT.
1.1.2 Previous flights
The occurrence pilot’s 2 previous flights of the day were also captured by the video camera mounted on the Emergency Response and Operations Centre.
The 1st flight departed CYQT at approximately 1313 with the pilot and 1 forestry air attack officer on board. Immediately after takeoff on Runway 12, the pilot made a low-level steep turn to the left, coming within approximately 200 feet of the CYQT Control Tower.
The 2nd flight departed CYQT at approximately 1759 with the pilot and same forestry air attack officer on board. Immediately after takeoff on Runway 12, the pilot made a low-level steep turn to the left, similar to the turn on the 1st flight; however, this time the pilot flew behind the CYQT Control Tower, coming within 600 feet of it.
1.2 Injuries to persons
The pilot was the only person on board the occurrence flight. Table 1 presents a summary of injuries.
| Degree of injury | Crew | Passengers | Persons not on board the aircraft | Total by injury |
|---|---|---|---|---|
| Fatal | 1 | – | – | 1 |
| Serious | 0 | – | – | 0 |
| Minor | 0 | – | – | 0 |
| Total injured | 1 | – | – | 1 |
1.3 Damage to aircraft
The occurrence aircraft was destroyed.
1.4 Other damage
The aircraft’s collision with Runway 07 resulted in damage to several runway lights and produced deep scarring on the runway surface. The post-impact fire and residual fuel deteriorated the composition of the asphalt runway surface. Runway 07 was subsequently closed for 6 days until repairs were completed.
1.5 Personnel information
1.5.1 Pilot
| Captain | |
|---|---|
| Pilot licence | Airline transport pilot licence (ATPL) |
| Medical expiry date | 01 July 2022 |
| Total flying hours | 2662.7 |
| Flight hours on type | 230.6 |
| Flight hours in the 7 days before the occurrence | 11.3 |
| Flight hours in the 30 days before the occurrence | 55.8 |
| Flight hours in the 90 days before the occurrence | 181.6 |
| Flight hours on type in the 90 days before the occurrence | 181.6 |
| Hours on duty before the occurrence | 10.3 |
| Hours off duty before the work period | 15.0 |
The pilot held the appropriate licence and ratings for the flight in accordance with existing regulations. He held a Canadian airline transport pilot licence and a valid Category 1 medical certificate with no restrictions.
The pilot was hired by MAG Canada in February 2021 to conduct bird dog flight operations and had previous experience on aircraft equipped with engines similar to those on the Rockwell International 690B. His initial training on the Rockwell International 690B was completed on 02 April 2021 and he successfully completed his pilot proficiency check on 03 April 2021. In March 2021, the pilot completed a company 4-hour initial crew resource management (CRM) training course approved by Transport Canada. The course was provided to all flight operations personnel at MAG Canada and addressed both multi-crew and single-pilot operations.
The pilot attended and successfully completed a bird dog workshop provided by the Ontario Ministry of Northern Development, Mines, Natural Resources and Forestry in April 2021. The workshop consisted of 6 hours of ground school, 4 hours of simulator training, and 2 hours of bird dog training in the aircraft.
Based on a review of the pilot’s work and rest schedules, fatigue was not considered a factor in this occurrence.
1.5.2 Air traffic services
On the day of the occurrence, 7 air traffic controllers were in the CYQT Control Tower; 3 of them communicated with the occurrence pilot.
| Controller | Controller 1 (Flight 1) | Controller 2 (in training) (Flight 2 and occurrence flight) | On-the-job instructor (Flight 2 and occurrence flight) |
|---|---|---|---|
| Air traffic control licence rating(s) | Airport control | Area control Airport control (in training) | Airport control |
| Medical expiry date | 31 January 2022 | 31 December 2021 | 20 April 2022 |
| Initial qualification date | 08 October 2015 | 12 June 1991 | 18 July 2001 |
| Qualification date at CYQT | 08 October 2015 | Phase 4 training Started: 13 October 2020 | 09 February 2005 |
| Hours on duty before the occurrence | Off duty and not in the tower at the time of the occurrence (shift hours were from 0730 to 1530 on the day of the occurrence) | 5 hours 54 minutes | 5 hours 54 minutes |
| Hours off duty before the work period | 16 hours | 145.5 hours | 49.5 hours |
1.6 Aircraft information
The occurrence aircraft was manufactured by Rockwell International in 1977 and was referred to as an Aero Commander 690B. The aircraft type certificate is currently owned by Twin Commander Aircraft LLC.
The Aero Commander 690B is a pressurized, high-wing, twin-engine turboprop aircraft and has a retractable landing gear. The aircraft is certified for single-pilot operation and can carry up to 10 people.
The occurrence aircraft was originally equipped with 2 Honeywell TPE-331-5-251K turboprop engines. In December 2006, the aircraft was modified with 2 Honeywell TPE-331-10T-516K turboprop engines in accordance with Supplemental Type Certificate SA236CH.Footnote 3
A review of the occurrence aircraft’s journey and technical records did not reveal any outstanding defects with the aircraft that may have contributed to the occurrence.
| Manufacturer | Rockwell International |
|---|---|
| Type, model and registration | Aero Commander, 690B, C-GYLD |
| Year of manufacture | 1977 |
| Serial number | 11426 |
| Certificate of airworthiness | 06 August 2014 |
| Total airframe time | 7620.7 hours |
| Engine type (number of engines) | Honeywell TPE 331-10T-516K (2) |
| Propeller type (number of propellers) | Hartzell HC-B3TN-5FL (2) |
| Maximum allowable take-off weight | 10 325 pounds |
| Recommended fuel types | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A-1 |
1.6.1 Elevator trim system
Flight control (rudder, elevator, and ailerons) trim systems reduce the amount of manual input required from the pilot to maintain a desired flight attitude. The Aero Commander 690B elevator trim tab selection is accomplished by moving the elevator trim control wheel in the cockpit, which drives a series of cables, flex cables, and trim tab actuators. A failure of the elevator trim cable on this aircraft will result in the loss of any further trim input and the elevator trim tab to be locked in the previously selected position.
1.6.2 Weight and balance
The aircraft had approximately 2250 pounds of fuel on board and a total gross weight of 9827 pounds at the time of the occurrence, which is below the maximum certified take-off weight of 10 325 pounds. It was determined that the occurrence aircraft was operated within the allowable weight and centre-of-gravity limitations for the intended flight.
1.7 Meteorological information
The CYQT aerodrome routine meteorological report (METAR) issued for 2100 was as follows:
- Wind 180° true at 6 knots
- Visibility 20 statute miles
- Few clouds at 28 000 feet AGL
- Temperature 23 °C, dew point 14 °C
- Altimeter setting 29.89 inches of mercury
Weather was not considered a factor in this occurrence.
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
CYQT has an elevation of 654 feet above sea level. There are 2 runway surfaces: Runway 12/30 and Runway 07/25. Both have an asphalt surface. Runway 12/30 is 5297 feet long and 150 feet wide and Runway 07/25 is 7318 feet long and 200 feet wide. At the time of the occurrence, both runways were active.
The investigation determined that the runways, taxiways, and aprons were bare and dry at the time of the occurrence. Runway conditions were not considered a factor in this occurrence.
1.11 Flight recorders
The aircraft was not equipped with a flight data recorder or a cockpit voice recorder, nor was it required to be by regulation.
The occurrence aircraft was equipped with an automatic dependent surveillance-broadcast (ADS-B) system. The ADS-B is
a surveillance system that uses a global navigation satellite system, aircraft avionics, and ground and/or space-based infrastructure to accurately and quickly transmit flight information. This includes aircraft identification, position, altitude, and velocity between aircraft and air traffic control. This signal can be captured on the ground or in space for surveillance purposes (ADS-B-out) or on-board other aircraft for air traffic situational awareness (ADS-B-in) and airborne separation assistance.Footnote 4
The occurrence aircraft was also equipped with a Skynode S200, a GPS-based flight tracking unit that transmits, receives, and stores flight information such as the time, aircraft position, speed, heading, and altitude.
Both the ADS-B and Skynode S200 units were secured by TSB investigators and sent to the TSB Engineering Laboratory in Ottawa, Ontario, for data analysis.
1.12 Wreckage and impact information
The occurrence aircraft struck Runway 07 in an inverted, wings-level, 45° nose-down attitude, with forward speed and a high rate of descent. The aircraft burst into flames on initial impact and slid approximately 840 feet down the runway before coming to rest, facing a north-northeast direction. The aircraft was destroyed by the impact and post-impact fire, which consumed approximately 70% of the aircraft structure.
Inspection of the runway surface at the point of initial impact revealed scarring that was produced by both propellers. Propeller scars, damage to both propellers, and engine instrument analysis suggest that the propellers were turning and that both engines were producing significant power on initial impact.
An inspection of the cockpit area found the landing gear selector in the gear-up position. The left and right main landing gear were found retracted and the nose landing gear was extended. During normal operation, the nose gear remains locked in the retracted position using hydraulic system pressure. The nose gear is extended by removing the hydraulic pressure and the gear is then forced down by a coil spring. The loss of hydraulic system pressure during impact resulted in the extension of the nose gear.
The aileron, elevator, and rudder controls were inspected for continuity and no pre-impact anomalies were revealed. Inspection of the flap system was inconclusive due to excessive fire damage.
A failed elevator trim cable was found on site and was sent to the TSB Engineering Laboratory for inspection. The elevator trim tab was found to be in the approximate position for normal takeoff. Analysis of the failed elevator trim cable revealed that most of the wires that comprised the cable had failed before the impact as a result of excessive wear.
The remaining wires of this cable failed in a tensile/ductile overload mode. However, due to excessive fire damage, it could not be determined whether the remaining wires of the trim cable failed before impact or as a result of the impact.
An inspection of the occurrence aircraft’s seat rails was inconclusive due to fire damage and an inspection of the pilot’s seat pin engagement lock did not reveal any pre-impact anomalies. The rudder lock and control column lock were found stowed in their proper locations for flight.
Inspection of the occurrence site and wreckage did not reveal any indication of a bird strike or bird ingestion by the engines.
1.13 Medical and pathological information
According to information gathered during the investigation, there was no indication that the pilot’s performance was affected by medical, pathological, or physiological factors.
1.14 Fire
The occurrence aircraft was refuelled before the occurrence flight and had approximately 2250 pounds of Jet A-1 fuel on board, which fed the post-impact fire.
Two airport fire trucks responded to the accident and were on site approximately 1 minute and 15 seconds after impact. The fire fighting crew had the fire well under control approximately 1 minute and 30 seconds later. The emergency response to this accident was immediate; as a result, a portion of the airframe survived the fire and was useful to the investigation.
1.15 Survival aspects
While the emergency response was immediate, the accident was not survivable due to the severity of impact forces and the post-impact fire. The emergency locator transmitter activated on impact and was deactivated by TSB investigators after the occurrence.
1.16 Tests and research
The TSB laboratory completed an aircraft performance analysis using data from the video camera and Skynode S200 unit.
The Aero Commander 690B Pilot’s Operating Handbook states that the flaps are to be retracted for takeoff. The investigation revealed that flaps were in the retracted position for takeoff on the occurrence flight. The analysis revealed that, immediately after rotation, the aircraft pulled up into a steep climbing left turn resulting in a g force of 1.8. The aircraft continued to roll to an approximate 40° to 50° bank. The aircraft’s momentum resulted in the aircraft climbing to an altitude of approximately 45 feet AGL while continuing to roll into a descent and collision with the runway.
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP103/2021 – Video Analysis
- LP115/2021 – Examination of Control and Trim Cables
- LP119/2021 – Propeller Blade Fracture
- LP120/2021 – NVM Data Recovery – Skynode
- LP121/2021 – NVM Recovery – PEDS [personal electronic devices]
- LP130/2021 – Instruments Analysis
- LP019/2022 – Aircraft Performance Analysis
1.17 Organizational and management information
1.17.1 MAG Aerospace Canada Corp.
MAG Canada provides specialized air services such as aerial fire management, aerial imagery, air charters, and flight training. The company is based out of Dryden, Ontario, and has 8 sub-bases. It provides air services in accordance with Subpart 702 (Aerial Work) and Subpart 703 (Air Taxi Operations) of the Canadian Aviation Regulations (CARs) and operates a variety of aircraft, including 4 Aero Commander 690Bs.
MAG Canada is a Transport Canada-approved maintenance organization under which all company aircraft are maintained.
1.17.1.1 Bird dog flight operations
One of the services provided by MAG Canada is bird dog flight operations to assist the Ontario Ministry of Northern Development, Mines, Natural Resources and Forestry with fighting forest fires. One type of aircraft used to conduct bird dog flight operations is the Aero Commander 690B aircraft, which requires a crew of 2: the pilot and a forestry air attack officer. The forestry air attack officer provides expertise in directing and coordinating the aerial management of forest fires and helps the pilot manage the workload in the cockpit.
The bird dog crew will assess water-bombing routes for the water-bombing aircraft and, if necessary, direct the water-bombing aircraft toward areas that require fire suppression. The bird dog crew also coordinates the air attack with the firefighters on the ground to ensure that they are clear of the area before the water-bombing aircraft arrive. Depending on the size of the forest fire, the area may become congested with aircraft traffic and the bird dog crew will climb to a higher altitude to provide air traffic control for the water-bombing aircraft.
Another essential task of the bird dog crew is to determine the flight routes in and out of the forest fire area. The inherent nature of a bird dog flight is such that the pilot may need to conduct low-level manoeuvres, sudden turns, and steep climbs.
1.17.1.2 MAG Aerospace Canada Corp. standard operating procedures
Although not required by regulation, MAG Canada maintains a standard operating procedures (SOPs) manual,Footnote 5 which contains procedures the flight crew is required to follow to safely and effectively carry out flight operations. The SOPs manual was uploaded onto an electronic flight bag that was carried on board the occurrence aircraft.
The SOPs in effect at the time of the occurrence did not provide any specific climb-out procedures for day VFR takeoffs.
1.17.2 NAV CANADA
NAV CANADA was founded in 1996 and is a private, not-for-profit corporation. It is responsible for air navigation services in Canada, including aviation weather services, air traffic services (ATS), aeronautical information, and air navigation technology.
1.17.2.1 Air traffic services
NAV CANADA operates the CYQT Control Tower, providing ATC, airport advisory, weather briefing, and flight information. CYQT air traffic controllers provide clearances and instructions to all aircraft within the Class D control zone, including aircraft on taxiways and runways as well as those departing and approaching the airport under instrument flight rules and VFR, to ensure the safe movement of aircraft both on the ground and in the air.
1.17.2.2 Air traffic controller phraseology
Guidance on communications and phraseology is set out in NAV CANADA’s Manual of Air Traffic Services – Tower (MATS-TWR)Footnote 6 and the CYQT Control Tower Unit Operations Manual.Footnote 7 NAV CANADA also publishes various phraseology guides with a view to standardizing communications for various scenarios.Footnote 8
The investigation reviewed the communications between NAV CANADA and the occurrence pilot during the 2 flights before the occurrence flight. Table 5 is a summary of those exchanges.
| Flight | Phase | Communication exchange |
|---|---|---|
| Flight 1 | Just before takeoff (at 1312:04) | Controller 1: “Bird Dog one six zero, tower, line up runway one two, back track if required.” Occurrence pilot: “Line up twelve, taking the backtrack Bird Dog one six zero.” |
| (at 1312:20) | Controller 1: “Bird Dog one six zero, left turn on course, winds one nine zero at ten gusting fifteen, cleared takeoff runway one two.” Occurrence pilot: “Clear takeoff twelve, left turn on course, Bird Dog one six zero, thanks.” |
|
| Shortly after takeoff (at 1313:40) | Controller 1: “that was fantastic.” | |
| Moments later (at 1314:26) | Controller 1: “Thanks for the little show.” Occurrence pilot: “I can get closer if you’d like?” Controller 1: “Sure.” |
|
| Flight 2 | Just before takeoff (at 1759:00) | Occurrence pilot: “Thunder Bay Tower, Bird Dog at Foxtrot.” Controller 2 (in training): “Bird Dog one six zero from Foxtrot backtrack runway one two backtrack as required.” Occurrence pilot: “Line up twelve and it will be a left hand turn out.” |
| (at 1759:36) | Controller 2 (in training): ”Bird Dog one six zero, Tower, winds one eight zero at 14 cleared takeoff one two, left turn on course.” Occurrence pilot: “Cleared takeoff twelve left turn on course Bird Dog one six zero.” |
|
| (at 1759:46) | Occurrence pilot: “Get your camera ready if you’d like.” Controller 2 (in training): “Sure! Will do.” Occurrence pilot: “Do you want me north or south of the tower?” Controller 2 (in training): “Your choice I got the camera ready.” Occurrence pilot: “All right we’ll go south.” |
|
| Shortly after takeoff (at 1801:03) | Controller 2: (in training): “Bird Dog, tower, thanks for the show, next time I wanna be on board.” Occurrence pilot: “Be careful for what you wish for, somebody once nicknamed this thing the barf dog.” Controller 2 (in training): “(chuckles) I know.” |
|
| Occurrence flight | Just before takeoff (at 2106:10) | Occurrence pilot: “And tower, Bird Dog one six zero coming up to Foxtrot, ready when able.” Controller 2 (in training): “Bird Dog one six zero, from Foxtrot back track as required, line up runway one two.” Occurrence pilot: “ Line up twelve Bird Dog one six zero.” |
| (at 2109:17) | Controller 2 (in training): “Bird Dog one six zero, tower, left or right turn on departure your choice, winds one nine zero at 6 cleared takeoff runway one two.” Occurrence pilot: “Cleared takeoff twelve and I’ll do the left turn out again, Bird Dog one six zero.” Controller 2 (in training): “Roger.” |
1.17.2.3 Safety management system
NAV CANADA has a Transport Canada-approved safety management system (SMS). NAV CANADA describes its SMS to be effective, efficient, fully integrated, and the driving force behind every decision that is made.Footnote 9
NAV CANADA has a number of proactive and reactive processes intended to improve safety by identifying and mitigating risks in the air navigation system. These processes are outlined in the NAV CANADA Safety Management System Manual.Footnote 10 Effective safety management includes proactive and reactive processes that serve to identify hazards and maintain risk at a level that is as low as reasonably practicable. The 2 types of processes are complementary; proactive processes help to identify hazards before initiating changes to an operation, while reactive processes help to identify unanticipated safety issues following the implementation of a change.
Relevant to this investigation, the Safety Management System Manual details that information is gathered from Aviation Occurrence Reports (AORs)(for reactive processes), and from the voluntary internal confidential reporting system, known as the ARGUS+ Program (which allows both proactive and reactive processes to be conducted).
1.17.2.4 Reporting and internal investigation
The mandatory AOR procedure is provided to ATS personnel in NAV CANADA’s Aviation Occurrence Reporting ProceduresFootnote 11manual. This manual contains 48 categories of reportable occurrences, 16 of which deal with regulatory or potential regulatory infractions. The 32 remaining categories of reportable occurrences are related to hazards to aviation. One category in particular states “[a]ny other event which is irregular, unplanned or nonroutine in nature which has known adverse effect upon flight safety or a major impact on operations.”Footnote 12
Controllers may also report non-routine events (NRE) as outlined in the MATS-TWR.Footnote 13 NRE reports are recorded in NAV CANADA’s Safety Information System. Employees are encouraged to report their safety concern to their manager. If they are not satisfied with the results of their concern, the employee can report to the ARGUS+ Program for further action.
Following this occurrence, NAV CANADA generated an AOR,Footnote 14 which categorized the occurrence as an accident. A review of the AOR concluded that all procedures were in accordance with NAV CANADA’s MATS-TWR and no internal investigation was required. The report was closed.
The TSB investigation determined that, post-occurrence, NAV CANADA management was made aware that atypical communication took place between air traffic controllers and the occurrence pilot earlier on the day of the occurrence. NAV CANADA had identified a trend of previous departures where the occurrence pilot was executing a steep turn immediately after departure. No AOR or NRE reports were generated regarding these events. Although there was concern the aircraft demonstrated a trend, NAV CANADA was satisfied that the controllers did not solicit the occurrence pilot's behaviour. According to NAV CANADA, its role is primarily the provision of ATS; identifying unusual flight manoeuvres is outside its training and scope.
1.18 Additional information
1.18.1 Pilot decision making and risk perception
Pilot decision making (PDM) is a cognitive process used to select a course of action between alternatives. Several factors, circumstances, and biases can affect PDM, including the flight objective or goal, and the pilot’s knowledge, experience, and training. Footnote 15 These factors can result in a pilot operating an aircraft beyond the aircraft's capability or beyond the pilot’s abilities.
Risk is a function of likelihood and adverse consequence. Risk perception is a component of PDM; it is the recognition of the inherent risk in a situation. Pilots’ risk perception can be altered by their relative experience of a situation; therefore, “situations that present a high level of risk for one person may present only low risk for another.” Footnote 16 Additionally, pilots who have experienced more hazardous situations tend to have a lower perception of risk when compared to pilots who have fewer experiences with hazardous situations. Footnote 17
Individuals who repeatedly perform a dangerous activity with no, or few, adverse consequences may become desensitized or habituated to the high level of risk. Problems can arise when perceived risks no longer match the actual risks associated with an activity.
1.18.2 Accelerated stall
An aerodynamic stall occurs when the wing’s angle of attack exceeds the critical angle at which the airflow begins to separate from the wing. When a wing stalls, the airflow breaks away from the upper surface, and the amount of lift generated is reduced to below that needed to support the aircraft.
The speed at which a stall occurs is related to the load factor of the manoeuvre being performed. The load factor is defined as the ratio of the aerodynamic load acting on the wings to its gross weight, and represents a measure of the stress (or load) on the structure of the aircraft. By convention, the load factor is expressed in g.
In straight and level flight, lift is equal to weight, and the load factor is 1g. In a banked level turn, however, greater lift is required. It can be achieved, in part, by increasing the angle of attack (by pulling back on the stick/elevator control), which increases the load factor. As the load factor increases with bank angle, there is a corresponding increase in the speed at which the stall occurs. A stall that occurs at a higher speed as a result of a high load factor, such as bank angle increased beyond 30°, is called an accelerated stall.
Accelerated stalls are usually more severe than unaccelerated stalls, and are often unexpected. As an example, a stall from a steep bank angle (greater than 30°) can result in one wing stalling before the other, leading to a spin and the aircraft rapidly losing altitude.
2.0 Analysis
The analysis will focus on the sequence of events, pilot decision making and risk perception, communications between pilots and air traffic controllers, occurrence reporting at NAV CANADA, and the elevator trim cable failure.
2.1 Accident scenario
The accident sequence was captured by a video camera mounted on the Emergency Response and Operations Centre at the Thunder Bay Airport (CYQT). In addition, data captured by the automatic dependent surveillance-broadcast (ADS-B) system and Skynode S200 flight tracking units from the occurrence aircraft were successfully downloaded and analyzed.
The occurrence pilot was instructed to line up and hold on Runway 12 to accommodate an incoming aircraft for landing. While holding, the occurrence pilot and the pilot of the incoming aircraft—who knew each other—had brief communications. The incoming aircraft then landed on Runway 25 and the occurrence pilot was cleared for takeoff on Runway 12.
Immediately after rotation, the occurrence pilot selected the landing gear up to reduce drag and then conducted a rapid, climbing, steep left-bank turn, possibly attempting to perform a low-level flyby of the incoming aircraft that was now taxiing in an east-northeast direction on Taxiway A. When the aircraft entered the rapid, climbing, steep-bank turn, heightened g forces resulted in an increased wing load, and the aircraft entered an accelerated stall at an altitude from which a recovery was not possible.
Finding as to causes and contributing factors
After takeoff from Runway 12 at CYQT, as the pilot conducted a rapid, low-level, climbing steep turn, the aircraft entered an accelerated stall that resulted in a loss of control and subsequent collision with the surface of Runway 07 in an inverted attitude.
2.2 Pilot decision making and risk perception
Individuals who repeatedly perform a dangerous activity with no, or few, adverse consequences, may become desensitized or habituated to a high level of risk. Problems can arise when perceived risks no longer match the actual risks associated with an activity. When pilots perform manoeuvres nearing the limits of the aircraft performance without adverse consequences, they can unintentionally drift beyond these limits on a subsequent flight. The occurrence pilot had performed steep low-level turns on previous flights, without any adverse consequences.
Bird dog operations involve conducting low-level manoeuvres, sudden turns, and steep climbs. The pilot was, therefore, frequently exposed to higher-risk flight manoeuvres. Although the pilot was likely aware of the potential consequences of too steep of a turn at low-level, he likely became desensitized to the likelihood that these consequences would occur.
Finding as to causes and contributing factors
The decision to conduct the rapid, low-level, climbing steep turn was likely influenced by an altered perception of risk from previous similar takeoffs that did not result in any adverse consequences.
2.3 NAV CANADA
2.3.1 Communications between pilots and air traffic controllers
The occurrence pilot engaged in atypical communications with 2 CYQT air traffic controllers on 2 previous flights on the day of the occurrence. On these 2 flights, the occurrence pilot performed a steep left turn on takeoff, laterally flying the aircraft to within 200 and 600 feet, respectively, of the control tower.
On the 1st flight, the controller appears to have initiated the communication shortly after the aircraft took off as a spur-of-the-moment reaction to having observed an unusual flight manoeuvre. The controller then responded to the pilot in a way that could encourage riskier behaviour.
On the 2nd flight, the controller responded to communications initiated by the occurrence pilot before takeoff. Shortly after the takeoff, the controller re-engaged the communication. In these communications with the occurrence pilot, the controller used words that could further encourage risky behaviour.
Air traffic controllers may not be fully cognizant of the potential adverse consequences that engaging in atypical communications could have on safety or of the unusual flight manoeuvres that these types of communications could encourage. These types of communications could act as a primer for subsequent behaviours.
Finding as to risk
If air traffic controllers engage in communications that may be perceived by pilots to encourage unusual flight manoeuvres, pilots may perceive this encouragement as a confirmation that the manoeuvres are acceptable to perform, increasing the risk of an accident.
2.3.2 NAV CANADA occurrence reporting
NAV CANADA reporting criteria includes 32 categories of reportable occurrences related to hazards to aviation. One of those describes an occurrence that is irregular, unplanned or non-routine, which has a known adverse effect on flight safety or a major impact on operations.
Air traffic controllers are not trained on or thoroughly knowledgeable of an aircraft’s performance limits. Therefore, controllers cannot necessarily make a distinction between an unusual flight manoeuvre and an unsafe or hazardous one, and identifying such manoeuvres is deemed to be outside the scope of the controllers’ role. However, a departure that intentionally comes within 200 feet of a control tower is an unusual flight manoeuvre that could reasonably be perceived to be of higher risk than a standard departure. A review of the aviation occurrence report issued following this occurrence concluded that all procedures complied with the Manual of Air Traffic Services – Tower, and no internal investigation was required. Therefore, a reactive investigation was not performed.
Finding as to risk
If NAV CANADA’s reporting procedures do not contain specific criteria for situations where air traffic services personnel perceive aircraft to be conducting unsafe flight manoeuvres, there is a risk that these manoeuvres will continue and result in an accident.
2.4 Elevator trim cable failure
A failed elevator trim cable was found at the occurrence site. It was determined that most of the wires that comprised this cable had failed before the impact due to excessive wear. However, given that the trim tab actuator and trim tab remained in the normal take-off position, the excessive wear did not affect the elevator trim position on the occurrence flight and did not contribute to the accident.
Finding: Other
Most of the wires that comprised the elevator trim cable failed before the impact as a result of excessive wear; however, this did not contribute to the occurrence because the trim tab remained in the normal take-off position.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- After takeoff from Runway 12 at Thunder Bay Airport, Ontario, as the pilot conducted a rapid, low-level, climbing steep turn, the aircraft entered an accelerated stall that resulted in a loss of control and subsequent collision with the surface of Runway 07 in an inverted attitude.
- The decision to conduct the rapid, low-level, climbing steep turn was likely influenced by an altered perception of risk from previous similar takeoffs that did not result in any adverse consequences.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If air traffic controllers engage in communications that may be perceived by pilots to encourage unusual flight manoeuvres, pilots may perceive this encouragement as a confirmation that the manoeuvres are acceptable to perform, increasing the risk of an accident.
- If NAV CANADA’s reporting procedures do not contain specific criteria for situations where air traffic services personnel perceive aircraft to be conducting unsafe flight manoeuvres, there is a risk that these manoeuvres will continue and result in an accident.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- Most of the wires that comprised the elevator trim cable failed before the impact as a result of excessive wear; however, this did not contribute to the occurrence because the trim tab remained in the normal take-off position.
4.0 Safety action
4.1 Safety action taken
4.1.1 MAG Aerospace Canada Corp.
Following the occurrence, MAG Aerospace Canada Corp. (MAG Canada) took the following safety actions:
- On 18 August 2021, issued a Maintenance Memo requiring an inspection of the pilot seat locking mechanism and seat rails on all MAG Canada Aero Commander 690 and 500 aircraft.
- On 19 August 2021, issued a Flight Operations Memo reminding pilots to ensure that their seat lock is positively engaged with the seat rail before engine start and once again before beginning the take-off roll.
- On 21 August 2021, suspended all flight operations and held a company-wide Safety Stand-Down meeting that was attended by all employees. Safety topics covered during these sessions included:
- MAG Canada’s safety policy;
- Compliance with standard operating procedures and safe practices;
- Normalization of deviance and acceptance of unsafe practices;
- The need for eradication of a “cowboy” or “hot dog” culture in the aviation community;
- Reiteration of the company’s anonymous, non-punitive safety reporting program; and
- A refresher on how to submit an anonymous hazard report.
- On 28 August 2021, issued a Flight Operations Memo implementing enhanced training on engine failures during the take-off roll and at the most critical flight stage. All MAG Canada Aero Commander 690 pilots underwent this training, which covered both on-ground and in-air materials.
- Invited the SMS Director of its U.S. affiliate, MAG Aero, to conduct an audit of its safety management system (SMS). The audit included a review of the company’s SMS as well as interviews with key personnel. No significant or non-compliant findings were found, and recommendations for improvement areas were reported to management.
- Updated its crew resource management (CRM) training materials to include more information on managing stress and internal/external pressures as well as the normalization of deviance. This material will be covered with in all future initial and recurrent CRM training.
- Issued an amendment to its Company Operations Manual. The amendment included new sections on day visual flight rules minimum altitudes and distances, and permissible low-altitude flight to reiterate the regulations under sections 602.14 and 602.15 of the Canadian Aviation Regulations.
- On 30 November 2022, issued an in-house service bulletin (MAG-2022-SB-001) specifying scheduled inspections of trim cables and pulleys at station 386.82 of their Twin Commander 690 aircraft. The inspections are to be completed by using a borescope camera, as current visual inspections are inadequate due to poor accessibility of the area.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .