Collision with terrain
Tyax Air Service Limited
de Havilland DHC-2 MK. I (Beaver), C-GIYV
Pemberton Aerodrome, British Columbia, 52 NM NNW
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At 1021 Pacific Daylight Time on 17 July 2022, the Tyax Air Service Limited float-equipped de Havilland DHC-2 MK. I (Beaver) aircraft (registration C-GIYV, serial number 1488) departed Tyaughton Lake, British Columbia, for a visual flight rules flight to Lorna Lake, British Columbia, with 1 pilot and 5 passengers on board. At approximately 1040, during cruise, the pilot attempted a course reversal in a valley, and the aircraft subsequently collided with terrain. The pilot and 2 of the passengers received serious injuries while 3 passengers received minor injuries. The aircraft was substantially damaged. The 406 MHz emergency locator transmitter activated but search and rescue efforts were delayed by approximately 3 hours due to low ceilings near the accident site.
1.0 Factual information
1.1 History of the flight
At 1021Footnote 1 on 17 July 2022, the Tyax Air Service Limited float-equipped de Havilland DHC-2 MK. I (Beaver) aircraft departed Tyaughton Lake, British Columbia (BC), for a visual flight rules (VFR) flight to Lorna Lake, BC, with 1 pilot and 5 passengers on board. This was the pilot’s 3rd round-trip flight of the day: the 1st flight was to Warner Lake, BC, and the next 2 flights had planned destinations of Lorna Lake. The flight to Warner Lake was uneventful. On the 2nd flight of the day, the pilot diverted to a different destination, Spruce Lake, BC, because of reduced visibility in the valleys and clouds that were obscuring the mountain passes near Lorna Lake.

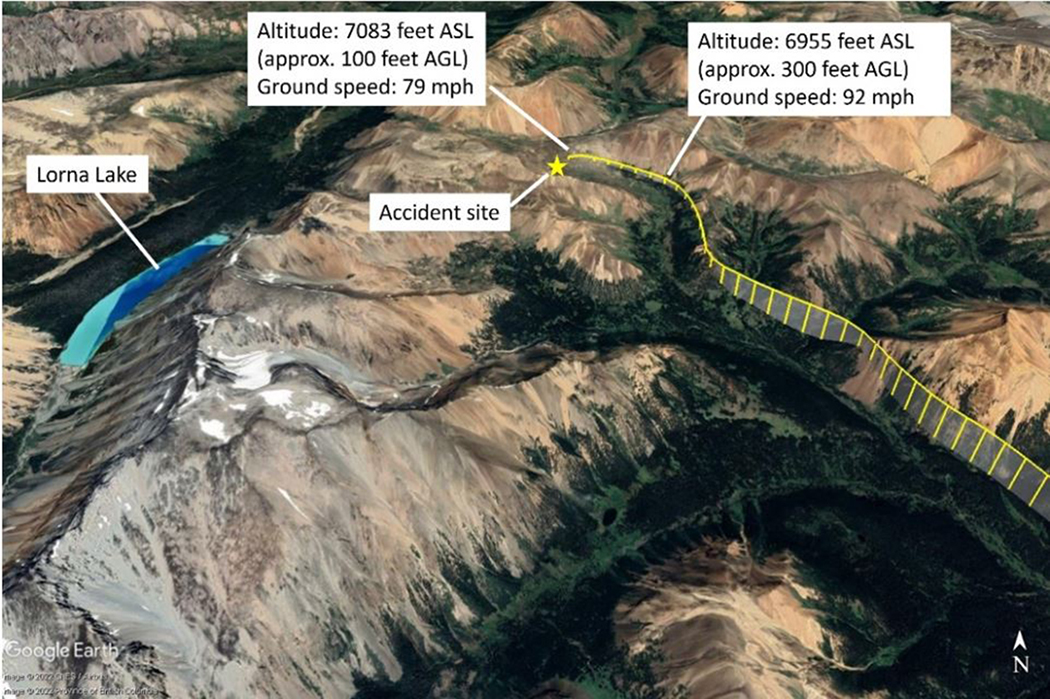
When flying through the valley toward Elbow Pass on the occurrence flight, the pilot, taking into account her experience on the previous flight, kept to the right side of the valley, slowed to approximately 100 mph, and extended the flaps to the climbFootnote 2 setting in anticipation of a course reversal. The airspeed further reduced to approximately 80 mph as the aircraft was approaching Elbow Pass, and there was increasing low cloud (Figure 1) that would prevent the aircraft from remaining clear of cloud over the pass; therefore, the pilot initiated a left turn to reverse course. The aircraft was flying at approximately 100 feet above ground level (AGL) at the time.
The pilot banked the aircraft to the left. During the left turn, the aircraft’s airspeed decreased (Figure 2). The pilot applied full power, the stall warning horn sounded,Footnote 3 and a few seconds later, at 1041, the aircraft collided with the down-sloping terrain.
The 406 MHz emergency locator transmitter activated, but search and rescue efforts were delayed due to low ceilings near the accident site. The 1st rescue helicopter arrived at the accident site at 1254. All occupants were evacuated by helicopters; the pilot and 1 passenger were transported to hospital in Kamloops, BC, and the remaining 4 passengers were transported to hospital in Whistler, BC.Footnote 4
1.2 Injuries to persons
The aircraft was configured with 3 rows of seating; the 1st row had 2 seats, the middle row had 3 seats, and the 3rd row had 1 seat.
Three of the 6 persons on board received serious injuries.
The pilot, who was seated in the front-left seat, received serious injuries, including injuries to the head and neck. The middle-row passengers received various injuries, including head injuries; a broken neck; bruising; and cuts to the head, arms, and hands that required stitches.
| Degree of injury | Crew | Passengers | Persons not on board the aircraft | Total by injury |
|---|---|---|---|---|
| Fatal | 0 | 0 | – | 0 |
| Serious | 1 | 2 | – | 3 |
| Minor | 0 | 3 | – | 3 |
| Total injured | 1 | 5 | – | 6 |
1.3 Damage to aircraft
The aircraft was substantially damaged.
1.4 Other damage
There was no other damage.
1.5 Personnel information
| Pilot licence | Airline transport pilot licence – aeroplane |
|---|---|
| Medical expiry date | 01 June 2023 |
| Total flying hours | 3028.2 |
| Flight hours on type | 76.8 |
| Flight hours in the 24 hours before the occurrence | 3.5 |
| Flight hours in the 7 days before the occurrence | 29.5 |
| Flight hours in the 30 days before the occurrence | 62.1 |
| Flight hours in the 90 days before the occurrence | approximately 135 |
| Flight hours on type in the 90 days before the occurrence | 76.8 |
| Hours on duty before the occurrence | 3.7 |
| Hours off duty before the work period | 13.5 |
The pilot held the appropriate licence and ratings for the flight in accordance with existing regulations. She held an airline transport pilot licence – aeroplane with a valid Category 1 medical certificate and a Group 1 instrument rating. She also had a seaplane rating and had accumulated 699.6 hours on floats. Although the pilot had not completed a mountain flying course, she had experience flying in the mountainous region of Nunavut, and the operator had spent extra time training her since this was her 1st job that involved flying in this region of mountains in BC.
The pilot had received 9.4 hours of flight training in June 2022. The training was provided by Tyax Air Service Limited in the occurrence aircraft and in an area with mountainous terrain that was similar to where the occurrence took place. The training included stalls, steep turns, and course reversals; however, given that no passengers or cargo were on board during these training flights, the aircraft’s weight during these training exercises was well below that during the occurrence flight in which the aircraft was fully loaded and close to the maximum gross weight.
Based on a review of the pilot’s work and rest schedule, there was no indication that the pilot’s performance was degraded by fatigue.
1.6 Aircraft information
| Manufacturer | de Havilland Aircraft of Canada Ltd.* |
|---|---|
| Type, model, and registration | DHC-2 MK. I, C-GIYV |
| Year of manufacture | 1961 |
| Serial number | 1488 |
| Certificate of airworthiness | 02 June 1992 |
| Total airframe time | 14 771.1 hours |
| Engine type (number of engines) | Pratt & Whitney USA, R-985-39 (1) |
| Propeller type (number of propellers) | Hartzell HC-B3R30-4B (1) |
| Maximum allowable take-off weight | 5370 pounds (2435.8 kg) |
| Recommended fuel type(s) | 80/87 octane minimum grade aviation gasoline |
| Fuel type used | 100 LL |
* Viking Air Ltd. is the current type certificate holder of the de Havilland DHC-2 MK. I (Beaver) aircraft.
The DHC-2 MK. I (Beaver) is a single-engine, high-wing, propeller-driven aircraft. The occurrence aircraft (Figure 3) was equipped with EDO 679-4930 floats.
![Occurrence aircraft (Photo: Peter J. Cooper, Beaver Tailsat https://dhc-2.com/id498.htm [last accessed on 28 March 2024].)](/sites/default/files/eng/rapports-reports/aviation/2022/a22p0057/images/a22p0057-figure-03.jpg)
The most recent maintenance, which consisted of a fuel pump replacement and avionics wiring repair, was performed 65.1 hours before the accident. There were no recorded defects outstanding at the time of the occurrence, nor was there any indication that a component or system malfunction played a role. The aircraft's weight and centre of gravity at the time of departure were within the prescribed limits.
Even though it was not required by regulation, the aircraft was equipped with a stall warning system, including a stall warning horn, that had been installed in 2018 in accordance with Supplemental Type Certificate (STC) 92-45. The aircraft was also equipped with several modifications, including a wing leading edge cuff to lower stall speed and a modification to engine mounts and battery location to improve flight characteristics, as well as upgraded handles on the aft doors and push out windows to assist with egress.
The occurrence aircraft was powered by a 9-cylinder Pratt & Whitney R-985 supercharged, radial, air-cooled engine and was equipped with a portable Garmin Aera 796 GPS (global positioning system) for its navigation equipment. It was not fitted with a radio altimeter, nor was it required to be by regulation.
1.7 Meteorological information
1.7.1 Forecast weather
According to the graphic area forecast (GFA) issued at 0426 and valid at 0500 on the date of the occurrence, the weather in the area near the accident site was forecast to be:
- Generally broken ceilings based at 3000 to 5000 feet above sea level (ASL), with tops at 10 000 feet ASL
- Visibility more than 6 statute miles (SM)
- Occasional altocumulus castellanus clouds with tops at 20 000 feet ASL and visibility of 5 SM to more than 6 SM in light rain showers and mist
- In valleys, localized visibility of 1 SM in mist with ceilings of 400 feet AGL
The GFA issued at 1025, shortly after departure, and valid at 1100 indicated a higher broken ceiling (with bases at 6000 feet ASL and tops at 14 000 ASL) and visibility of more than 6 SM. The clouds changed from altocumulus castellanus to towering cumulus, but the tops, visibility, and weather associated with these clouds remained the same. This GFA indicated that localized ceilings had increased to 1200 feet AGL, but it also included isolated cumulonimbus clouds with tops at 32 000 feet ASL and visibility of 5 SM in moderate thunderstorms and rain, with winds gusting to 25 knots.
In the absence of a reported barometric pressure setting, the pilot set the aircraft altimeter to the elevation of Tyaughton Lake before departing on the occurrence flight.
1.7.2 Meteorological assessment
After the accident and at the request of the TSB, Environment and Climate Change Canada performed an in-depth analysis of the weather conditions affecting the flight routing and the area surrounding the accident site at the time of the occurrence.
The meteorological assessmentFootnote 5 determined that on the morning of the occurrence, the route between Tyaughton Lake and Lorna Lake was “under the influence of a departing, weak low-pressure system, and an impending ridge of high pressure, giving a slack pressure gradient in the southern regions of BC.”Footnote 6 Although satellite images showed signs of convection in the area, it would have been weak with low cloud tops and associated with a slight chance of rain showers and a low risk of turbulence.
The analysis also stated that moderate northwesterly surface winds, with some gusts near 20 knots, were likely present in the area. These winds followed the valley and were dependent on the surface pressure gradient. However, above the peaks of the surrounding mountains, the winds were no longer guided by the terrain and therefore took on a different direction, southerly or southwesterly, at a similar strength. This shift in wind direction likely produced an area of wind shear at the meeting point of these different wind patterns, near mountaintops. While this wind shear would be considered light, a small aircraft, such as the occurrence aircraft, could still have been affected.Footnote 7
Environment and Climate Change Canada further described the winds and their effect on the aircraft at the time of the occurrence:
[G]iven the rough and complex terrain, surface winds forced through valleys may have been strong enough to generate local moderate mechanical turbulence or low-level wind shear below mountaintops.
Within the cloud over the crash location, surrounding stations reported ceilings in the 5000 – 9000 ft ASL range, with some scattered 600-foot AGL ceilings. Given the elevation of the incident (near 7100 feet [ASL]), this cloud deck would have likely been observed much [closer] to the surface, and could easily have resulted in cloud ceilings below 1000 feet AGL, with surrounding peaks obscured.Footnote 8
In spite of the scarcity of observations, the analysis concluded that the most likely conditions on the occurrence aircraft’s route between Tyaughton Lake and Lorna Lake were cloudy with low ceilings (possibly lower than 1000 feet AGL) in the vicinity of higher terrain, with obscured mountain peaks, and an abrupt change in wind direction as the aircraft ascended toward them, which could have had an impact on the occurrence flight.Footnote 9
1.7.3 Wind shear and downdrafts
The Transport Canada Aeronautical Information Manual defines wind shear as a “change in wind speed and/or wind direction in a short distance.”Footnote 10 It notes that wind shear “can exist in a horizontal or vertical direction and occasionally in both.”Footnote 11 When wind is forced over a mountain range, waves may form on the lee side of the mountains. These lee waves produce prominent downdrafts close to the mountain.
Although the exact winds at the time of the occurrence are unknown, winds in mountain ranges can be very unpredictable and downdraftsFootnote 12 are not uncommon. As explained in Mountain Flying,
[w]hen wind blows over large mountain ridges, the wind blowing up the windward slope, in a stable atmosphere, is usually relatively smooth. However, it spills rapidly down the leeward side, setting up strong downdrafts and causing turbulence in a situation which can be compared to water flowing down a rough stream bed. These downdrafts may be dangerous and can place an aircraft in a position from which it might not able to recover.Footnote 13
In addition, as explained in Weather Ways, “[i]n general, the strength of the downdrafts is such that an aircraft flying parallel to the range could be forced to the ground or, if flying upwind, might fail to clear the range.”Footnote 14
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
Not applicable.
1.11 Flight recorders
The aircraft was not equipped with a flight data recorder or a cockpit voice recorder, nor was either required by regulation.
The occurrence aircraft had a Garmin Aera 796 GPS on board; however, due to the significant damage to the aircraft after the collision, staff at the TSB Engineering Laboratory in Ottawa, Ontario, were unable to extract any data from the unit.
The aircraft was equipped with a Latitude Technologies flight tracking unit, which was also sent to the TSB Engineering Laboratory for analysis. Although it provided detailed information about the aircraft’s flight path, the exact altitude and coordinates could not be determined because of errors associated with the data. Footnote 15
1.11.1 TSB Recommendation A18-01
Information gathered from lightweight flight-data recording systems can be crucial to understanding the sequence of events leading to an aircraft’s collision with terrain. Flight data recorders can reliably capture such data as altitude, heading, airspeed, and other aircraft parameters, often at 1-second intervals, while cockpit voice recorders can record radio transmissions and other sounds from the cockpit, such as occupants’ voices and engine noises.
Following an occurrence on 13 October 2016, in which a Cessna Citation 500 aircraft collided with the ground after entering a steep descending turn and all occupants were fatally injured, Footnote 16 the Board recommended that
the Department of Transport require the mandatory installation of lightweight flight recording systems by commercial operators and private operators not currently required to carry these systems.
TSB Recommendation A18-01
In its December 2023 response to Recommendation A18-01, Transport Canada (TC) indicated that it agrees in principle with the recommendation.
TC stated that it was reassessing the approach and scope of the lightweight data recorders requirements and will produce a new revised Notice of Proposed Amendment (NPA). Additionally, TC has extended the deliverable dates for publishing the new NPA for consultation with industry stakeholders into fiscal year 2024–25.
TC also stated that it will establish a timeline for publication of the NPA in the Canada Gazette, Part I after the review of stakeholder comments. TC did not provide a timeline for the subsequent revision of the NPA and publication of the final NPA in the Canada Gazette, Part II. Based on the previous implementation periods identified in TC’s September 2021 response, it is likely that any regulatory change would take many years to be implemented.
In the TSB assessment of TC’s response, the Board remained concerned with the potential change in approach and scope of the lightweight data recorders requirements and the lengthy delays in implementation. Until the revised NPA is available for review, it is unknown if the previously proposed requirements will be preserved.
Therefore, in February 2024, the Board indicated that it was unable to assess the response to Recommendation A18-01.Footnote 17
This recommendation remains Active.
1.12 Wreckage and impact information
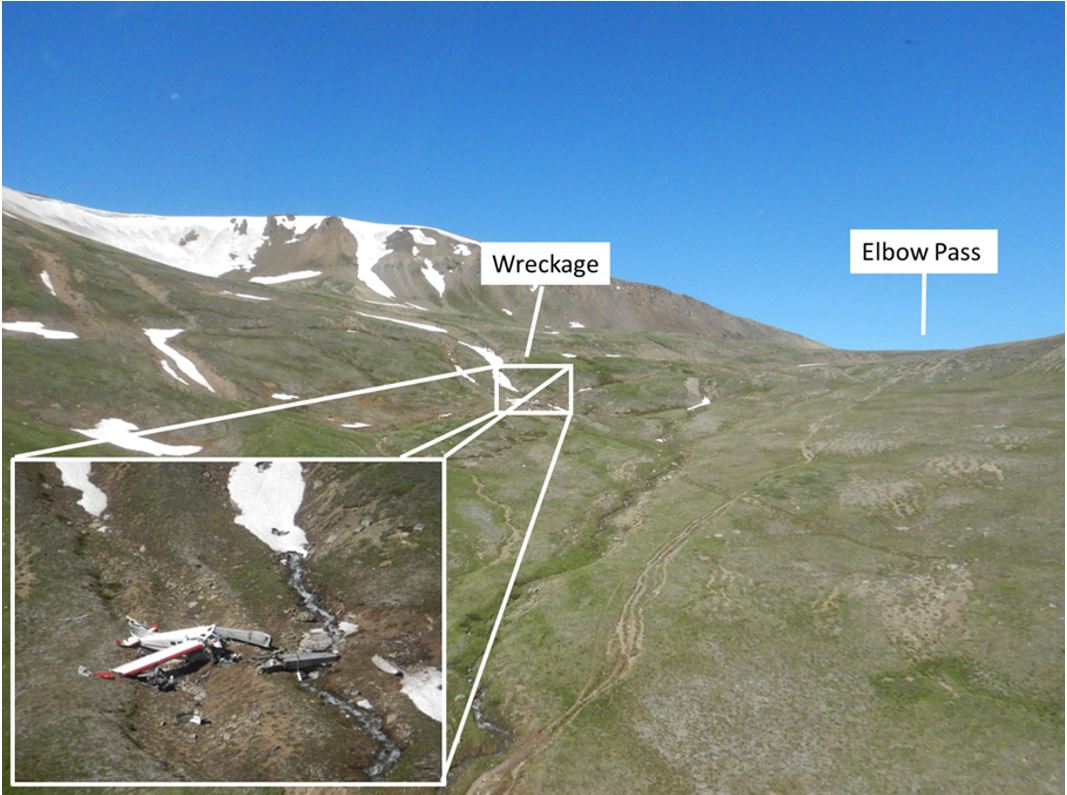
During the collision, the left float struck the ground first, then the aircraft pitched nose down and turned 180° to the left, coming to rest facing the opposite direction of travel, approximately 126 feet from the initial point of impact. Propeller ground scars were visible near the initial impact point. The ground scars and damage to the propellers were consistent with the engine producing power at the time of impact. The floats, left wing, and engine separated from the fuselage (Figure 4).
1.13 Medical and pathological information
According to information gathered during the investigation, there was no indication that the pilot’s performance was affected by medical factors.
1.14 Fire
There was no indication of fire either before or after the occurrence.
1.15 Survival aspects
1.15.1 Safety belts
The aircraft’s 2 front seats were equipped with a safety belt consisting of a lap strap combined with a shoulder harness; the rear seats were equipped with a lap strap only. All occupants were wearing their lap straps, and the occupants of the 2 front seats were also wearing the available shoulder harnesses.
The use of a safety belt, including a shoulder harness is known to reduce the severity of upper-body and head injuries and more evenly distribute impact forces.Footnote 18
1.15.1.1 TSB Recommendation A13-03
The TSB has previously recommended (TSB recommendations A94-08 and A92-01) that small commercial aircraft be fitted with seatbelts and shoulder harnesses in all seating positions. Following these recommendations, changes to regulations were made to require shoulder harnesses in all commercial cockpits and on all seats in aircraft manufactured after 1986 with 9 or fewer passengers. Footnote 19 This regulatory change did not address the vast majority of the commercial floatplane fleet, which was manufactured prior to 1986.
The TSB considers that, given the additional hazards associated with accidents on water, such as not being able to exit the aircraft due to incapacitation, shoulder harnesses for all seaplane passengers will reduce the risk of incapacitating injury, thereby improving the likelihood of exiting the aircraft.
As a result of TSB investigation A12O0071, the Board recommended that:
The Department of Transport require that all seaplanes in commercial service certificated for 9 or fewer passengers be fitted with seatbelts that include shoulder harnesses on all passenger seats.
TSB Recommendation A13-03
TC indicated in its January 2014 response to the recommendation that it did not agree with the recommendation, stating that the structures and interior designs of these older aircraft are not robust enough to support shoulder restraints and may hinder egress. Also, in its latest response in September 2020, TC stated that better occupant restraint “would not produce a significant reduction in fatalities and would not offset the cost of modifying multiple models of seaplanes to install shoulder harnesses.” Footnote 20 TC does not plan to take further action in response to this recommendation.
The TSB’s reassessment of TC's response in March of 2021 states that the risk presented by inadequate occupant restraint is well known to exist, is reflected in current airworthiness standards, was found to have caused or contributed to fatal injuries in previous TSB investigations and was detailed in safety studies completed by both the TSB and the Federal Aviation Administration of the United States. Therefore, it was not clear why TC indicated that, because the relative influence of this hazard cannot be quantified precisely, action will not be taken to address the safety deficiency. Therefore, the Board considered the response to Recommendation A13-03 to be Unsatisfactory.
The TSB recommendation is currently Dormant. Footnote 21
Accident experience has provided substantial evidence that use of a shoulder harness in conjunction with a lap strap can reduce serious injuries to the head, neck, and upper torso of aircraft occupants and has the potential to reduce fatalities of occupants involved in an otherwise survivable accident.
The benefits of shoulder harnesses are described in the Federal Aviation Administration’s Advisory Circular 21-34 as follows:
Shoulder harness-safety belt systems prevent serious head, neck, and upper torso injuries in what may be relatively minor accidents in terms of aircraft damage, and they can prevent irreversible or fatal injuries in more severe accidents. Therefore, the major benefits of shoulder harnesses occur in an accident environment, but they can be of no benefit if they are not available for use in an accident. Footnote 22
1.15.2 Satellite communicator
One passenger on board the occurrence aircraft had a compact satellite communicator. This device was used to contact emergency services following the collision with terrain.
1.15.3 Survival equipment
The investigation revealed that no survival equipment had been carried on board the aircraft during the occurrence flight. Following the collision with terrain, parts of the aircraft’s interior, emergency blankets, and clothing the passengers had carried in their packs, as well as the packs themselves, were all used to block the wind and keep the occupants warm while they waited for emergency services to arrive. First aid kits from the aircraft and the passengers’ packs were used to administer first aid.
For a flight to be exempt from the Canadian Aviation Regulations (CARs) requirement for aircraft to carry survival equipment when operated within 25 nautical miles (NM) of the aerodrome of departure, the pilot must have the “capability of radiocommunication with a surface-based radio station for the duration of the flight.” Footnote 23 The flight from Tyaughton Lake to Lorna Lake is less than 25 NM, but the occurrence aircraft was incapable of very high frequency (VHF) radiocommunication with the dispatcher at Tyax Lodge Footnote 24 while it was on Lorna Lake because of the region’s mountainous terrain. Footnote 25 Therefore, the aircraft was required to carry survival equipment.
1.16 Tests and research
1.16.1 Aircraft turn performance analysis
The TSB laboratory conducted an aircraft performance analysis on the course reversal that the occurrence aircraft had conducted before it impacted the terrain. Based on recorded groundspeed data, the aircraft’s average airspeed as it initiated the course-reversal turn was calculated to be 73.2 mph.Footnote 26
Computer modelling of the aircraft’s turn performance was completed based on the aircraft flight manual, data extracted from the flight tracker, and information provided by the aircraft manufacturer.
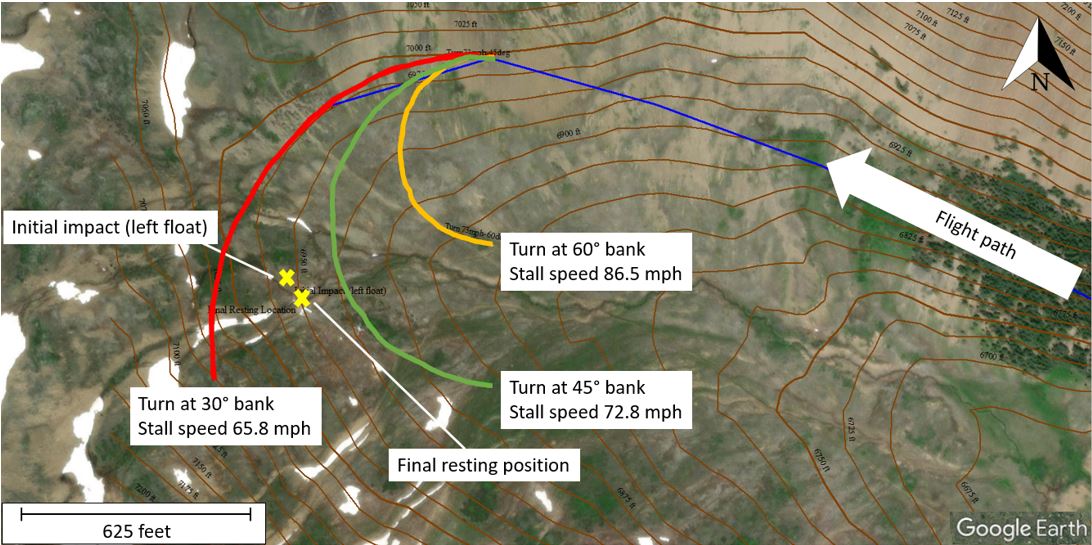
Results from the modelling included turn radius and stall speed calculations. In the image (Figure 5) that the test produced, the course-reversal turn depicted in green (at 45° bank) indicates a successful turn, while the one depicted in yellow (at 60° bank) indicates an aircraft stall. The turn shown in red (at 30° bank) indicates that the aircraft would have run out of available space in the valley.
However, the analysis shows that at an airspeed of 73.2 mph, it is possible that the course-reversal turn may have been successful at a bank angle of 45°.
The occurrence aircraft was not equipped with a flight data recorder and, therefore, the aircraft’s actual angle of bank and airspeed during the course-reversal turn were unavailable.
1.16.2 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP064/2022 – NVM Recovery – GPS and Flight Tracker
- LP040/2023 – Aircraft Performance Analysis
1.17 Organizational and management information
At the time of the occurrence, Tyax Air Service Limited held an air operator certificate issued by TC. It operated under CARs subparts 702 (Aerial Work) and 703 (Air Taxi Operations) and conducted flights primarily for the tourism industry. It was based at Tyaughton Lake and operated aircraft on floats, wheels, and skis. The occurrence flight was being operated under CARs Subpart 703.
Single-pilot operations were based on self-dispatch at Tyax Air Service Limited. Consequently, decisions to depart and decisions to continue a flight were made by the pilot based on information obtained and what was observed at the time.
At the time of the accident, Tyax Air Service Limited operated only the occurrence aircraft, and at the time of publication of this report, the operator had voluntarily surrendered its air operator certificate.
1.18 Additional information
1.18.1 TSB air transportation safety issue investigation report on air-taxi operations in Canada
In 2019, the TSB published Safety Issue Investigation (SII) Report A15H0001. Footnote 27 The objective of this SII was to improve safety by reducing the risks in air-taxi operations across Canada. The air-taxi sector continues to experience more accidents and more fatalities than any other in the commercial aviation industry.
Phase 1 of the SII included an examination of 167 TSB investigation reports involving both fixed-wing and rotary-wing aircraft. This examination found that most fatalities involved flights that had begun in visual meteorological conditions, continued through the loss of visual references, and ended in either controlled flight into terrain or a loss of control. An analysis of accident data found that contributing factors fell into 2 broad areas:
- acceptance of unsafe practices; and
- inadequate management of operational hazards.
In phase 2 of the SII, investigators conducted interviews with industry stakeholders to better understand the pressures faced by the industry, as well as the issues encountered in daily activities. The information gathered was organized into 19 safety themes which, after further analysis using additional data, yielded various conclusions. Of the 19 themes, the following 4 and their respective conclusions are relevant to this report:
- Acceptance of unsafe practices, which can lead to an increased risk of an accident if they are not recognized and mitigated, or if they are accepted over time as the “normal” way to conduct business.
- Operational pressure, which can take the form of internal and external pressures, including pressure to get the job done, and can negatively impact safety.
- Training of pilots and other flight operations personnel, which is essential for them to develop the skills and knowledge they need to effectively manage the diverse risks associated with air-taxi operations.
- Pilot decision making/crew resource management, which are critical competencies that help flight crews manage the risks associated with aircraft operations.
1.18.2 Visual flight rules obstacle clearance
The occurrence flight was conducted in accordance with CARs Subpart 703. Section 703.27 of the CARs states:
Except when conducting a take-off or landing, no person shall operate an aircraft in VFR flight
- at night, at less than 1,000 feet above the highest obstacle located within a horizontal distance of three miles from the route to be flown; or
- where the aircraft is an aeroplane, during the day, at less than 300 feet AGL or at a horizontal distance of less than 300 feet from any obstacle.Footnote 28
The aircraft was not equipped with a radio altimeter,Footnote 29 nor was it required to be by regulation.Footnote 30 While the lack of radio altimeter might not have contributed directly to the accident, a radio altimeter could have improved the pilot’s awareness of the aircraft’s height above ground when the turn was initiated at approximately 100 feet AGL.
1.18.3 Course-reversal procedures
TC’s publication Take five… for safety: Flying VFR in the Mountains provides the following pointer: “Don’t fly in the middle of a valley. Fly on one side and make sure that a safe turning radius is available. Always have an escape route open [emphasis in original].”Footnote 31
When turning back in a narrow canyon, pilots should stay to one side and start the turn from as close to that side of the canyon as possible, and turn using the minimum radius appropriate for the aircraft. During the turn, pilots will normally reduce speed, extend partial or full flaps and then roll to about 45° of bank. At the same time, they will select full power and apply back pressure as needed to maintain the aircraft in level flight. If a pre-stall warning is received, or buffeting is felt, pilots should reduce the bank angle only enough to stop the warning. Once the turn is done, pilots will set the flaps and throttle back to the normal settings for cruising flight.Footnote 32
1.18.4 Human factor issues
1.18.4.1 Pilot motivation and operational pressure affecting decision making
As documented in the SII, a pilot’s direct contact to passengers is a typical feature of most air-taxi operations. Compared to airline pilots operating under CARs Subpart 705 (Airline Operations), an air-taxi pilot’s interaction with passengers is more extensive and may likely include greeting passengers on arrival, collecting passenger data for weight and balance calculations, delivering safety briefings, fitting life preservers, discussing the flight plan (including alternates and weather constraints), organizing cargo, arranging passenger seating, and interacting with passengers during the flight.
This close interaction with the passengers can affect the pilot’s ability to make safe decisions and manage risks effectively once airborne. Since the direct nature of the pilot’s role begins with customer service before performing the operational role of flying the aircraft, air-taxi pilots are more likely to be aware of the reasons the passengers are travelling. This knowledge may influence the pilot’s decision making and risk management. This operational pressure can influence the pilot’s natural decision-making process, including the decision about whether a plan is still sound, or whether a different course of action is necessary.
Because the pilot was unable to reach the original destination of Lorna Lake on the previous flight, she was motivated to achieve the goal of successfully finding a route to the destination, thereby creating a mental model, which is an intrinsic component of decision making. Mental models are internal representations that allow an individual to describe, explain, and predict events or situations in their environment.Footnote 33 When a mental model is adopted, it generates expectations and is resistant to change. This leads to increased internal operational pressure to continue the flight. Compelling new information must be absorbed to modify a mental model.
1.18.4.2 Mountain navigation and visual cues
In mountain flying, dispersed trees or shrubs function as visual cues that characterize valley dimensions. Observable vegetation can aid in estimating the aircraft’s height above ground.
In addition, trees or bushes allow pilots to effectively confirm both their distance from the terrain and the relative size of the mountain in comparison. These factors aid the pilot in estimating whether a course reversal can be safely
conducted.Footnote 34
Given that the upper valley leading to Elbow Pass is uniform in contour with no discernible vegetation in the surrounding area, the pilot had fewer visual cues on which to rely while flying in the valley.
1.18.4.3 Personal safety minima
Personal minima are an individual pilot’s set of limits and guidelines used in making decisions that may be more conservative than what the regulations require. According to the Federal Aviation Administration, “personal minimums should be set so as to provide a solid safety buffer between the skills required for the specific flight [a pilot] want[s] to make, and the skills available to [the pilot] through training, experience, currency, and proficiency.”Footnote 35 To accomplish this, pilots should review the regulatory minima, assess their experience and comfort level, set a baseline for personal minima, adjust for specific conditions, and then stick to the plan.Footnote 36
For example, within the specific context of mountain flying under VFR, TC recommends that pilots establish an altitude that they will need in order for the aircraft to clear the pass or ridge at the end of a valley.Footnote 37 This altitude might vary from pilot to pilot, depending on each pilot’s personal safety minima and the buffer they wish to maintain.
Although the CARs can stipulate the minimum regulatory limits, pilots can set their own personal safety minima that go beyond these regulatory limits. Establishing hard personal limits can help pilots to increase their safety margins.
1.18.4.4 Flight operations in rain
Rain on the aircraft’s windscreen adds to the visual clutter that can obscure outside references available to a pilot, increasing the pilot’s workload in visual scanning and perception.

Depending on their size and density, water droplets carried by the relative airflow across windscreens of aircraft unequipped with wiper systems, such as the occurrence aircraft, may obscure the pilot’s forward view (Figure 6). This obscured view prompts the pilot’s need to visually process windscreen contamination to see beyond it and complicates the task of estimating the aircraft’s height above ground and distance from cloud. The visual processing of the windscreen contamination requires the use of cognitive resources and adds to the time required for effective aircraft handling and timely decision making while manoeuvring in confined areas.
The Transport Canada Aeronautical Information Manual further explains the difficulties of flight operations in rain:
An error in vision can occur when flying in rain. The presence of rain on the windscreen, in addition to causing poor visibility, introduces a refraction error. This error is because of two things: firstly, the reduced transparency of the rain-covered windscreen causes the eye to see a horizon below the true one (because of the eye response to the relative brightness of the upper bright part and the lower dark part); and secondly, the shape and pattern of the ripples formed on the windscreen, particularly on sloping ones, which cause objects to appear lower. The error may be present as a result of one or other of the two causes, or of both, in which case it is cumulative and is of the order of about 5° in angle. Therefore, a hilltop or peak 1/2 NM ahead of an aircraft could appear to be approximately 260 ft lower, (230 ft lower at 1/2 SM) than it actually is.
Pilots should remember this additional hazard when flying in conditions of low visibility in rain and should maintain sufficient altitude and take other precautions, as necessary, to allow for the presence of this error. Also, pilots should ensure proper terrain clearance during en route flight and on final approach to landing.Footnote 38
2.0 Analysis
The investigation did not identify any issues related to pilot licensing or aircraft system malfunctions that contributed to this occurrence. As a result, the analysis will focus on the circumstances and conditions under which the occurrence flight was conducted.
In particular, the analysis will explore the human factor issues that contributed to the continuation of the flight into the valley and toward the intended destination of Lorna Lake. It will then describe the elements of the course-reversal turn that contributed to the aircraft’s impact with terrain. The risks associated with not carrying survival equipment or data recorders will also be discussed.
2.1 Human factor issues
2.1.1 Pilot decision making
Given the level of connection that most Canadian Aviation Regulations (CARs) Subpart 703 pilots have with day-to-day operations, pilot decision making within the context of air-taxi operations is tightly coupled with the objective of the flight. As documented in Safety Issue Investigation Report A15H0001, a pilot’s direct contact to passengers is a typical feature of most air-taxi operations. As a result, goal conflicts may arise as the pilot works toward accommodating passengers while also working to absorb operational delays due to weather, late passengers, and administrative duties.
2.1.2 Motivation
The occurrence pilot conducted 3 round-trip charter flights on the day of the occurrence from Tyaughton Lake, British Columbia (BC): the 1st flight was to Warner Lake (BC) and the next 2 flights were planned to Lorna Lake, BC. The 1st flight arrived at Warner Lake as planned, the 2nd flight diverted to a different destination owing to clouds and weather conditions near Lorna Lake, and the 3rd was the occurrence flight. While the operator was supportive of decisions made by pilots to divert or return to base due to safety concerns such as low or impassable weather conditions, the pilot was motivated to achieve the goal of successfully finding a route to the destination and felt increased internal operational pressure to continue the flight.
As the pilot entered the valley with the intention of navigating toward Lorna Lake, the clouds and weather she observed appeared to allow for continued visual flight rules (VFR) flight along the route over Elbow Pass and into Lorna Lake. The plan was to explore the feasibility of using Elbow Pass as a means to get to Lorna Lake.
Because the weather conditions had forced the pilot to divert on the 2nd flight, seeking out a navigable route to the planned destination on the occurrence flight was the pilot’s primary goal. The pilot’s mental model, which was based on the unsuccessful 2nd flight and the expectation that improved weather would allow for success, created and reinforced her expectations of potential success on the occurrence flight.
The result was that the pilot was motivated and likely experienced some internal operational pressure to complete the occurrence flight as planned.
Finding as to causes and contributing factors
As the aircraft entered the valley, the pilot decided that the visibility and cloud height were sufficient to continue the VFR flight toward the planned destination. This was likely motivated by internal operational pressures resulting from a previous unsuccessful flight and the underlying aspiration to reach the planned destination.
Owing to the fact that the pilot had to divert to another location on the 2nd flight of the day, the pilot realized that a course reversal may be required during the occurrence flight.
Finding as to causes and contributing factors
Anticipating the requirement for a course reversal, the pilot configured the aircraft to increase manoeuvrability and positioned it on the right side of the valley. As a result, the aircraft was operating close to the ground, at a speed closer to its stall speed.
2.1.3 Reduced visual cues nearing Elbow Pass
2.1.3.1 Valley terrain
In mountain flying, dispersed trees or shrubs act as a visual cue that can define the dimensions of a valley. The upper valley leading to Elbow Pass is above the treeline and uniform in contour, with no discernible vegetation in the surrounding area that could have served as a visual cue to the pilot. Consequently, it was more difficult to discern the valley’s dimensions and, therefore, more difficult to determine whether she could safely reverse course.
2.1.3.2 Precipitation
While entering the valley leading into Elbow Pass, the aircraft was operating in VFR conditions below an overcast layer of cloud and in precipitation. Photographs taken on the day of the occurrence show precipitation on the aircraft windscreen.
Rain on aircraft windscreens can obscure outside references available to a pilot, making visual scanning and perception more difficult and time-consuming. Water droplets streaming across an aircraft’s windscreen may obscure the pilot’s forward view, complicating the already complex task of estimating the aircraft’s height above ground and distance from cloud. The need to visually process windscreen contamination can draw the pilot’s cognitive resources away from the crucial tasks of flying the aircraft and making decisions while manoeuvring in confined areas, such as valleys.
Finding as to causes and contributing factors
As the aircraft continued toward Elbow Pass, the pilot’s perception of the aircraft’s position relative to clouds, the ground, and other physical features was influenced by the presence of water droplets on the windshield and the unavailability of various visual cues in the valley. As a result, it was difficult for the pilot to detect the abruptly rising terrain and the substantially reduced height above the ground, which delayed the initiation of the course reversal.
2.2 Factors affecting a course-reversal turn
2.2.1 Weather
In the morning, before the 1st flight of the day, the pilot had reviewed the weather conditions along the planned route. During the occurrence flight, she was aware of the weather conditions along the route because this was her 3rd flight of the day in the same area.
Clouds, winds, and obscuring phenomena can change quickly at the top of mountain passes and ridges, and when an opening or clearing in the clouds appears to present an opportunity for an aircraft to transit through, this opening can quickly disappear and leave a pilot to search for another escape route. The decision to reverse course in a mountain valley can be made at any point. However, when this decision is delayed in adverse or changing weather conditions, the options for a safe escape become less apparent, and safety margins are reduced.
Although the pilot had anticipated the possibility of a course reversal, the decision to complete the manoeuvre was made late and, consequently, the safe options for escape were reduced.
As the aircraft entered the turn, its airspeed decreased below 80 mph and the stall warning horn sounded. The pilot applied full power; however, the aircraft collided with terrain. A performance analysis completed during the investigation determined that a turn at 45° angle of bank at 73.2 mph should have been possible; however, the actual speed or angle of bank of the aircraft could not be determined, nor could the influence of possible downdrafts in the area.
Finding as to causes and contributing factors
The course reversal was initiated at approximately 100 feet above ground level at a reduced airspeed, which decreased further in the turn. The aircraft impacted the down-sloping terrain nearing the completion of the turn, likely as a result of a stall, a downdraft, or both.
2.2.2 Training
The pilot had developed a background in mountain flying based primarily on operations in Nunavut. Her contract with Tyax Air Service Limited was her 1st job in which she conducted flight operations in the mountains of BC.
The flight training that the pilot received covered stalls, steep turns, and course reversals. However, given that no passengers or cargo were on board during the training flights, the pilot did not conduct these manoeuvres and procedures with aircraft weights that were representative of operational flights, including the occurrence flight in which the aircraft was close to its maximum gross weight.
Finding as to risk
If a pilot’s in-flight training on stalls and course reversals is conducted at aircraft weights well below those of operational flights, there is a risk that the pilot will not recognize the limitations of the aircraft or how it will perform with realistic weights.
2.2.3 Incorporating personal safety minima
Pilots need to ensure that they maintain adequate ground clearance and distance from obstacles so that there is sufficient height available to execute a turn in the event of an emergency. For pilots operating under CARs Subpart 703, there is a requirement to maintain an altitude of 300 feet above ground level during daytime operations.
Transport Canada recommends that pilots determine, well before reaching the ridge at the end of a valley, the minimum altitude that will be required to clear it. If pilots set their own personal limits based on their level of comfort and experience with mountain flying, this will assist them in deciding on the minimum altitude to be flown and whether to reverse course if it cannot be maintained. Setting altitude limits by incorporating personal safety minima is a useful defence against many dynamic situations in flight, such as quickly changing weather and added operational and personal pressure.
Setting personal safety minima beyond regulatory limits can increase safety margins.
Findings as to risk
If pilots do not incorporate concrete personal safety margins into their operational work, there is a risk that they will operate beyond their skills and capabilities.
If air-taxi pilots operate an aircraft below the regulatory minimum of 300 feet above ground level, there is a risk that there may be insufficient height to safely complete emergency or evasive actions and collision with terrain may occur as a result.
2.3 Safety belts
Although the aircraft was equipped with safety belts, including shoulder harnesses in the cockpit, the passenger seats in the rear were equipped with lap straps only. Two of the passengers seated in these rear seats received injuries consistent with flailing or contact with the aircraft structure. It could not be determined if these injuries would have been prevented if shoulder harnesses had been available; however, the use of safety belts that include shoulder harnesses is known to reduce the severity of upper-body and head injuries, and more evenly distribute impact forces.
The TSB made a recommendation in 2013 calling for light seaplane aircraft, such as the occurrence aircraft, to be fitted with safety belts that included shoulder harnesses on all passenger seats. The recommendation was specifically targeted to address the possible effect of injury-related incapacitation on underwater egress; however, the risk of injury for passengers flying in light aircraft without shoulder harnesses, regardless of landing surface, remains elevated.
Finding as to risk
If light aircraft are not equipped with safety belts that include shoulder harnesses on all passenger seats, there is an increased risk of passenger injury as a result of flailing and/or contact with the aircraft structure.
2.4 Survival equipment
According to the CARs, if a flight is operated within 25 nautical miles of the aerodrome of departure and the pilot has access to radiocommunication with a surface-based radio station for the flight’s duration, the flight is exempt from the requirement to carry survival equipment. Although the occurrence flight route was less than 25 nautical miles, the aircraft was incapable of communicating with Tyax Lodge via radio while it was on Lorna Lake. Therefore, the exemption was not applicable, and the aircraft was required to carry survival equipment.
The investigation determined that the occurrence aircraft was not carrying any survival equipment. Following the collision with terrain, the passengers relied on aircraft parts and their own supplies to shield themselves from the wind and stay warm while waiting for emergency services. First aid kits from the aircraft and the passengers’ packs were used to administer first aid.
Owing to the fact that the accident occurred in mountainous terrain, rescue efforts were delayed owing to low ceilings near the site of the collision.
Finding as to risk
If aircraft are not equipped with survival equipment, there is a risk that accident survivors may not have sufficient means to treat injuries or manage harsh climate and weather conditions until rescued, increasing the risk of further injury or death.
2.5 Lightweight data recorders
The occurrence aircraft did not have a lightweight data recorder, nor was it required to by regulation. The TSB laboratory analyzed the aircraft performance, beginning from the course-reversal turn until the impact with terrain. Owing to the lack of data with respect to the aircraft’s angle of bank, airspeed, and engine parameters, the investigation was unable to determine the exact cause of the aircraft’s collision with terrain.
Finding as to risk
If commercial and private aircraft are not equipped with a lightweight data recorder, crucial flight data may not be available to investigators after an accident, increasing the risk of not being able to determine the underlying causes and advance transportation safety.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- As the aircraft entered the valley, the pilot decided that the visibility and cloud height were sufficient to continue the visual flight rules flight toward the planned destination. This was likely motivated by internal operational pressures resulting from a previous unsuccessful flight and the underlying aspiration to reach the planned destination.
- Anticipating the requirement for a course reversal, the pilot configured the aircraft to increase manoeuvrability and positioned it on the right side of the valley. As a result, the aircraft was operating close to the ground, at a speed closer to its stall speed.
- As the aircraft continued toward Elbow Pass, the pilot’s perception of the aircraft’s position relative to clouds, the ground, and other physical features was influenced by the presence of water droplets on the windshield and the unavailability of various visual cues in the valley. As a result, it was difficult for the pilot to detect the abruptly rising terrain and the substantially reduced height above the ground, which delayed the initiation of the course reversal.
- The course reversal was initiated at approximately 100 feet above ground level at a reduced airspeed, which decreased further in the turn. The aircraft impacted the down-sloping terrain nearing the completion of the turn, likely as a result of a stall, a downdraft, or both.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If a pilot’s in-flight training on stalls and course reversals is conducted at aircraft weights well below those of operational flights, there is a risk that the pilot will not recognize the limitations of the aircraft or how it will perform with realistic weights.
- If pilots do not incorporate concrete personal safety margins into their operational work, there is a risk that they will operate beyond their skills and capabilities.
- If air-taxi pilots operate an aircraft below the regulatory minimum of 300 feet above ground level, there is a risk that there may be insufficient height to safely complete emergency or evasive actions and collision with terrain may occur as a result.
- If light aircraft are not equipped with safety belts that include shoulder harnesses on all passenger seats, there is an increased risk of passenger injury as a result of flailing and/or contact with the aircraft structure.
- If aircraft are not equipped with survival equipment, there is a risk that accident survivors may not have sufficient means to treat injuries or manage harsh climate and weather conditions until rescued, increasing the risk of further injury or death.
- If commercial and private aircraft are not equipped with a lightweight data recorder, crucial flight data may not be available to investigators after an accident, increasing the risk of not being able to determine the underlying causes and advance transportation safety.
4.0 Safety action
4.1 Safety action taken
The Board is not aware of any safety action taken following this occurrence.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .